Urinary Tract Infections: History and Discovery
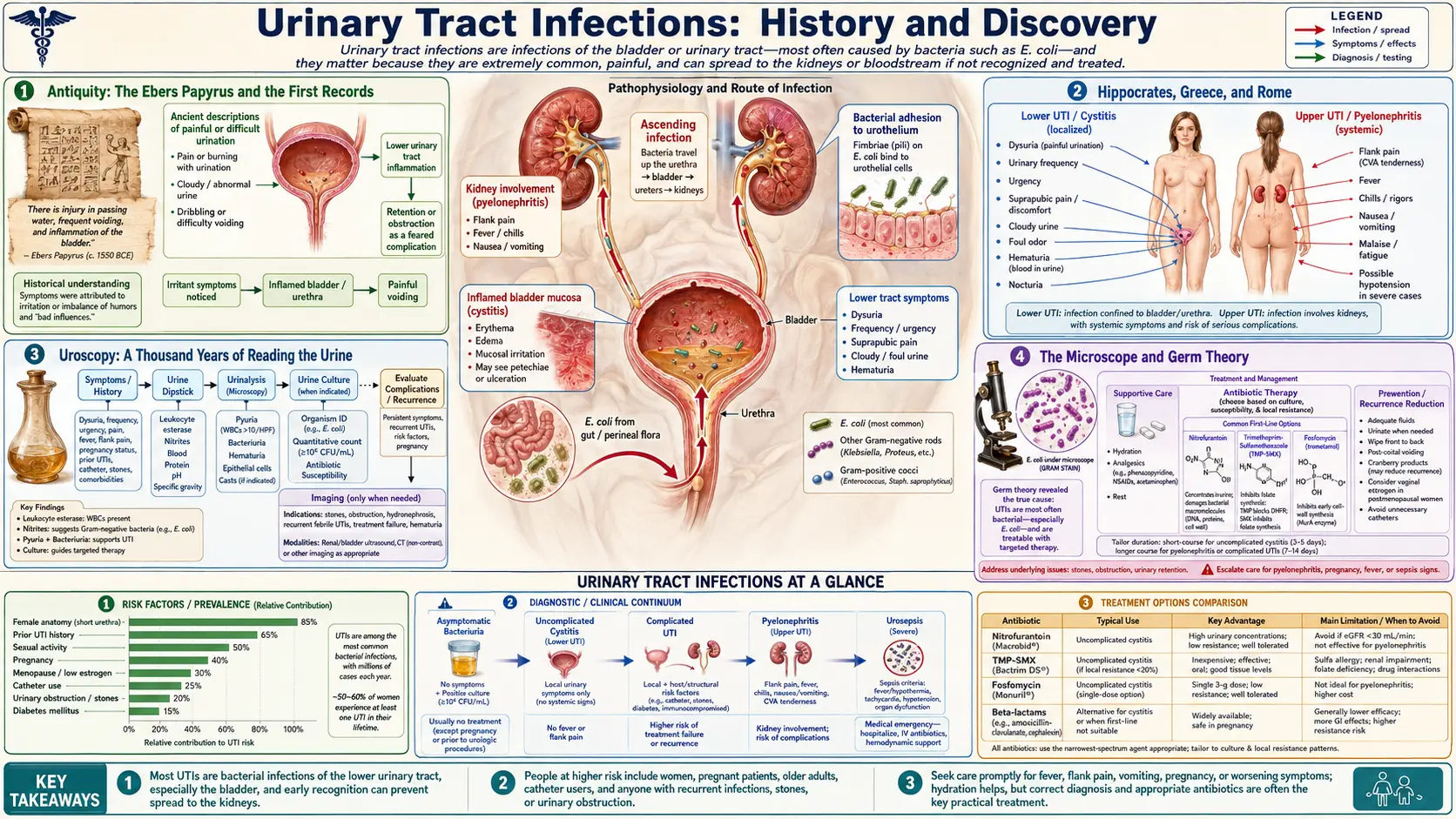
Urinary tract infections are almost certainly as old as humanity, and the written record of them stretches back nearly three and a half thousand years. Ancient physicians could not see the cause, but they knew the symptoms intimately — burning, frequent, urgent, and sometimes bloody urination — and they read disease in the urine itself. The Ebers Papyrus of Egypt (around 1550 BCE) describes the bladder "sending forth heat," the Hippocratic writers of Greece catalogued painful and obstructed urination, and for more than a thousand years European and Byzantine doctors held up the glass urine-flask to the light in the elaborate art of uroscopy. The true cause — living bacteria — came into view only with the microscope and germ theory in the nineteenth century, when Theodor Escherich isolated the organism we now call Escherichia coli in 1885. Edward Kass turned diagnosis into a number in 1956, and modern science has since uncovered why women are predisposed, how uropathogenic E. coli hides inside bladder cells, and why antibiotic resistance now threatens to undo a century of progress.
Table of Contents
- Antiquity: The Ebers Papyrus and the First Records
- Hippocrates, Greece, and Rome
- Uroscopy: A Thousand Years of Reading the Urine
- The Microscope and Germ Theory
- Theodor Escherich and the Discovery of E. coli (1885)
- Edward Kass and Significant Bacteriuria (1956)
- The Antibiotic Era and Rising Resistance
- Modern Understanding: Anatomy, Biofilms, and UPEC
- Cranberry and the Folk-Remedy Tradition
- Research Papers and References
- Connections
- Featured Videos
Antiquity: The Ebers Papyrus and the First Records
The earliest written descriptions of what we would now call a urinary tract infection appear in ancient Egypt. The Ebers Papyrus, a comprehensive medical scroll dated to around 1550 BCE, is among the oldest surviving medical documents in the world, and it contains passages that historians of medicine read as descriptions of urethritis, cystitis, and related bladder complaints. In one often-cited phrase, the papyrus describes the affliction as the bladder "sending forth heat" — an apt, plain-language account of the burning that anyone who has had a bladder infection will recognize instantly.
Egyptian medicine blended careful observation with magico-religious explanation. The same papyri that describe painful and bloody urination also attribute some urinary symptoms to "worms," and indeed in the Nile valley much hematuria (blood in the urine) was caused by Schistosoma haematobium, the parasite of urinary schistosomiasis — so the ancient association of bloody urine with "worms in the belly" was, for that disease, not entirely wrong. What matters for our story is that more than three thousand years ago, physicians were already recording the cardinal symptoms of urinary disease and attempting to treat them with herbal and mineral preparations.
Across the ancient world the urinary tract drew attention precisely because its disorders were so visible and so distressing. The symptoms — frequency, urgency, burning, retention, and blood — could be observed without dissection, and the urine could be collected, smelled, and inspected. This made the urinary tract one of the very first organ systems whose diseases were systematically described, long before anyone understood what an organ, a cell, or a germ actually was.
Hippocrates, Greece, and Rome
The Greek tradition associated with Hippocrates of Kos (c. 460–c. 370 BCE) and the texts of the Hippocratic Collection brought a more naturalistic eye to urinary disease. Hippocratic writers described and named the disorders of urination that still organize the field today: dysuria (difficult or painful urination), strangury (slow, drop-by-drop, painful urination), and retention of urine. They defined the symptoms of bladder stones — painful urination, blood, and obstruction — and they distinguished various forms of urinary difficulty by whether they were accompanied by severe pain, slight pain, or none.
Crucially, the Hippocratic physicians did not merely describe; they intervened. The Collection mentions urethral catheterization to relieve retention and the use of diuretics, and the famous Hippocratic Oath specifically forbids cutting for stone ("I will not cut, even for the stone"), leaving that dangerous operation to specialist lithotomists. The treatise On Airs, Waters, and Places — an early work of environmental medicine — held that the quality of a community's drinking water influenced the frequency of stone disease, gravel, and strangury, an observation that, while framed in humoral terms, reflects a genuine attempt to find external causes for urinary illness.
Roman and later Greco-Roman physicians, including the encyclopedists and the great compiler Galen, inherited and extended this body of knowledge. They refined the descriptions of urinary symptoms, developed bronze and metal catheters, and continued the practice of inspecting urine for signs of disease. Yet the fundamental limit remained: with no concept of microorganisms and no instrument to magnify the invisible, the ancient world could describe a urinary tract infection in exquisite clinical detail without ever knowing what caused it.
Uroscopy: A Thousand Years of Reading the Urine
If antiquity established the symptoms, the medieval world built an entire diagnostic system around the urine itself. Uroscopy — the visual inspection of urine for color, clarity, sediment, smell, and even taste — became the single most important diagnostic tool of medieval and Renaissance medicine, and for centuries the glass urine flask, the matula, was the very emblem of the physician, the way the stethoscope is today.
The intellectual foundations were laid by the Byzantine physician Theophilus Protospatharius, who in roughly the seventh century CE wrote De Urinis ("On Urines"), generally regarded as the first treatise devoted entirely to the study of urine. Later Byzantine authorities such as Joannes Actuarius (c. 1275–1328) expanded the doctrine, paying particular attention to urinary sediments — the cloudy deposits that we now recognize can contain the pus cells and bacteria of an infection. By the high Middle Ages, physicians compared a patient's specimen against elaborate color charts — the so-called urine wheel — that mapped twenty or more gradations of color and consistency onto specific diagnoses and prognoses.
Seen through modern eyes, uroscopy was a mixture of real signal and elaborate guesswork. A cloudy, foul-smelling, sediment-laden urine genuinely can indicate infection, and so some uroscopic judgments were sound. But the practice was pushed far beyond what inspection alone could reveal — into prognosis, character-reading, and outright divination — and by the early-modern period the spectacle of the "piss prophet" diagnosing any ailment from a flask alone had become a target of satire and reform. Still, uroscopy deserves real credit in this history: for well over a thousand years it kept the urine at the center of diagnosis, and its careful attention to sediment pointed, however dimly, toward the microscopic truth that the microscope would finally reveal.
The Microscope and Germ Theory
The decisive turn came when the human eye was finally extended into the invisible world. In the 1670s the Dutch draper and self-taught microscopist Antonie van Leeuwenhoek ground lenses of extraordinary power and became the first person to see and describe living bacteria and protozoa, which he called animalcules. For the first time, the tiny organisms that teem in water, saliva, and bodily fluids were visible — though no one yet connected them to disease, and nearly two centuries would pass before the link was made.
That link was forged in the second half of the nineteenth century by the founders of the germ theory of disease. Louis Pasteur showed that specific microorganisms drove fermentation and putrefaction and could cause disease; Robert Koch developed the rigorous methods — pure culture on solid media, staining, and microscopy — that allowed a particular microbe to be tied to a particular illness, and formalized the logical criteria now known as Koch's postulates; and Joseph Lister applied the new understanding to surgery through antisepsis. Once it was accepted that invisible living organisms cause infection, the burning, cloudy, foul urine that physicians had pondered for millennia suddenly had a candidate explanation: bacteria growing where they did not belong.
This was the intellectual and technical stage onto which the discovery of the chief urinary pathogen would step. The tools were now in place — the microscope to see the organism, pure-culture technique to isolate and grow it, and a theory that made sense of it all. What remained was for someone to find, name, and characterize the specific bacterium responsible for so many of these infections.
Theodor Escherich and the Discovery of E. coli (1885)
That someone was Theodor Escherich (1857–1911), a German-Austrian pediatrician working in Munich. Studying the bacteria of the infant intestine, in 1885 Escherich isolated from the stool of healthy infants a rod-shaped organism he named Bacterium coli commune — "the common colon bacterium" — and described its morphology and properties before the Society of Morphology and Physiology that same year. In 1919, after his death, the bacterium was renamed Escherichia coli in his honor; the name was formally adopted internationally in 1958. It is worth being precise about the historical record here: Escherich first described E. coli as a normal inhabitant of the healthy gut. Its central role as the leading cause of urinary tract infections was established by later clinical and microbiological work, not by Escherich's original 1885 papers.
The connection, however, follows naturally from where the organism lives. E. coli normally resides harmlessly in the colon, but because the openings of the digestive and urinary tracts sit close together — especially in women — gut bacteria are perfectly placed to migrate to the urethra and ascend into the bladder. Today, Escherichia coli is recognized as the single most common cause of urinary tract infections, responsible by most estimates for the large majority of uncomplicated cases. The everyday clinical fact that "most UTIs are caused by E. coli" rests directly on Escherich's identification of the organism, even though he himself was studying infant digestion rather than the bladder.
Escherich's work exemplifies how the germ-theory revolution turned a vague ancient affliction into a specific, nameable, treatable disease. Once the pathogen had a name and could be cultured, physicians could in principle ask the right questions: which organism is present, how many, and which treatment will kill it. Answering the second of those questions — how many — would take another seventy years and the work of Edward Kass.
Edward Kass and Significant Bacteriuria (1956)
Identifying the bacterium solved one problem but created another. The lower urethra is not sterile, and a voided urine sample inevitably picks up some bacteria on its way out. So a culture that grows some bacteria does not, by itself, prove infection — it might simply reflect contamination. How could a clinician tell a true bladder infection from a contaminated specimen? The answer came from the American physician Edward H. Kass at Harvard.
In a landmark report published in 1956 (in the Transactions of the Association of American Physicians), Kass introduced the concept of "significant bacteriuria." By quantitatively culturing urine — counting the colony-forming units (CFU) per milliliter — and comparing patients who had urinary infection with those who did not, he showed that a count of 105 (100,000) CFU/mL or greater reliably distinguished genuine infection from mere contamination. In his data, the great majority of patients with symptomatic infection exceeded this threshold, while contaminated specimens generally fell below it. Kass candidly described the cutoff as designated "arbitrarily" as the dividing line, but it worked, and it transformed diagnosis from a subjective judgment into an objective, reproducible number.
The "Kass criterion" of ≥105 CFU/mL standardized UTI diagnosis worldwide and underpinned the screening of asymptomatic populations — including pregnant women, in whom Kass showed that silent bacteriuria carried real risk. Remarkably, his threshold, derived from studies with relatively small sample sizes, has remained in use for roughly seventy years. Modern guidelines now refine it — recognizing that symptomatic women, particularly with organisms like E. coli, can be genuinely infected at much lower counts (e.g. 102–103 CFU/mL) — but the conceptual breakthrough of quantitative bacteriuria, and much of the framework still taught and used today, traces directly to Kass's 1956 work.
The Antibiotic Era and Rising Resistance
Knowing the cause and being able to diagnose it precisely meant little without a way to cure it — and that arrived with the antibiotic revolution of the mid-twentieth century. The sulfonamides of the 1930s were the first synthetic antibacterial drugs widely used against urinary infections, and because many are excreted in active form in the urine, they concentrate exactly where a UTI needs to be treated. Nitrofurantoin, an agent that concentrates in the urinary tract while keeping blood levels low, was approved in the United States in 1953 and became a mainstay of lower-UTI treatment. In the following decades the toolkit expanded with trimethoprim and the combination trimethoprim-sulfamethoxazole, the beta-lactams, and eventually the fluoroquinolones and fosfomycin.
For a generation, a urinary tract infection became a minor inconvenience: a short course of pills, and the burning was gone in days. This success is genuine and enormous — it is easy to forget that pyelonephritis (kidney infection) and urosepsis were once frequently fatal. But the very convenience of antibiotics, and their heavy use, set in motion the central problem of modern UTI care: antibiotic resistance. Because UTIs are so common and so often treated empirically (before culture results return), they have been a major arena for the evolution of resistant bacteria.
Resistance is now a defining theme. Uropathogenic E. coli increasingly carry resistance to the old first-line drugs, and strains producing extended-spectrum beta-lactamases (ESBLs) — which defeat many penicillins and cephalosporins — have spread globally, sometimes leaving few oral options. Stewardship efforts now push clinicians back toward narrow-spectrum, urine-concentrating agents like nitrofurantoin and fosfomycin for uncomplicated cystitis, to spare the broader-spectrum drugs. The history of UTI treatment has thus come full circle in a sobering way: having finally conquered an ancient affliction, medicine must now fight to keep the cure working.
Modern Understanding: Anatomy, Biofilms, and UPEC
Late-twentieth- and twenty-first-century research has filled in why UTIs happen, why women suffer them so much more often, and why they so stubbornly recur. The first piece is anatomy. The female urethra is far shorter than the male's, and its opening lies close to the vagina and anus, giving gut and skin bacteria a short, easy path into the bladder. This single fact — recognized and quantified by modern urology rather than ancient medicine — explains much of the dramatic sex difference in UTI rates, alongside contributing factors such as sexual activity, certain spermicides, pregnancy, and the hormonal changes of menopause.
The second piece is the discovery that the chief pathogen is not a passive passenger but an active invader. Specialized strains called uropathogenic E. coli (UPEC) are armed with hair-like surface fibers called type 1 pili, tipped with an adhesin protein called FimH that latches onto sugar (mannose) receptors on the bladder lining. Research led by Scott Hultgren and colleagues showed that, having attached, UPEC can invade the surface bladder cells and multiply inside them into dense, biofilm-like clusters known as intracellular bacterial communities (IBCs). Sheltered within the host's own cells, the bacteria are largely shielded from antibiotics and from the immune system, and they can later re-emerge — a compelling explanation for why some women endure infection after infection with the same organism.
This modern picture — short urethra, gut reservoir, FimH-mediated adhesion, cellular invasion, intracellular reservoirs, and biofilms — has opened genuinely new therapeutic ideas that go beyond simply killing bacteria. Anti-adhesion strategies (including FimH antagonists called mannosides, designed to block the bacterium from ever gripping the bladder wall) and vaccine approaches are under active investigation. The thread that began with the Ebers Papyrus — the bladder "sending forth heat" — now runs all the way to the molecular handshake between a pilus tip and a bladder-cell sugar.
Cranberry and the Folk-Remedy Tradition
No history of urinary tract infections is complete without the folk remedies people reached for long before antibiotics, and the most enduring of these is cranberry. North American Indigenous peoples used cranberries and related berries for food, dye, and medicine, and by the nineteenth and twentieth centuries cranberry juice had become a popular Western home remedy for "bladder trouble." For a long time its supposed benefit was attributed to acidifying the urine — an explanation that modern research has largely set aside.
The more credible mechanism emerged only recently. Cranberries are rich in A-type proanthocyanidins (PACs), and laboratory and ex-vivo studies indicate that these compounds can interfere with the adhesion of P-fimbriated and type-1-fimbriated E. coli to the cells lining the urinary tract — in effect, loosening the same molecular grip that the FimH research illuminated. This gives the old folk remedy a plausible, mechanistic rationale rooted in exactly the pathophysiology modern science has uncovered: if the bacteria cannot stick, they are flushed away with the urine before they can establish an infection.
The clinical evidence, however, must be presented honestly and cautiously. Cranberry is not a treatment for an established infection — an active UTI needs proper medical assessment and, usually, antibiotics — and the trial data on prevention have been genuinely mixed for years, muddied by inconsistent product potency and study quality. A 2023 Cochrane systematic review pooling roughly fifty trials concluded that cranberry products probably do reduce the risk of recurrent UTIs in certain groups, such as women with recurrent infections and children, while finding little benefit in others (for example, the elderly or those with bladder-emptying problems). The fair summary is that cranberry is a reasonable, low-risk preventive option for some people prone to recurrent UTIs — a long-standing folk practice that modern evidence partially, but not unconditionally, supports.
Research Papers and References
The list below combines key peer-reviewed papers and reviews on the history, microbiology, and pathophysiology of urinary tract infections with curated PubMed topic-search links into the broader historical literature. Ancient primary sources (the Ebers Papyrus, the Hippocratic Collection, and Theophilus' De Urinis) are named in the article as historical texts rather than as modern citations. Where a stable DOI or PubMed identifier is available it is linked directly; otherwise a PubMed topic search is provided. Each link opens in a new tab.
- Kass EH. Asymptomatic infections of the urinary tract. Transactions of the Association of American Physicians. 1956;69:56-64. — Search PubMed
- Shulman ST, Friedmann HC, Sims RH. Theodor Escherich: the first pediatric infectious diseases physician? Clinical Infectious Diseases. 2007;45(8):1025-1029. — doi:10.1086/521946
- Friedmann HC. Escherich and Escherichia. EcoSal Plus. 2014;6(1). — doi:10.1128/ecosalplus.ESP-0025-2013
- Justice SS, Hung C, Theriot JA, et al. Differentiation and developmental pathways of uropathogenic Escherichia coli in urinary tract pathogenesis. PNAS. 2004;101(5):1333-1338. — doi:10.1073/pnas.0308125100
- Anderson GG, Palermo JJ, Schilling JD, Roth R, Heuser J, Hultgren SJ. Intracellular bacterial biofilm-like pods in urinary tract infections. Science. 2003;301(5629):105-107. — doi:10.1126/science.1084550
- Flores-Mireles AL, Walker JN, Caparon M, Hultgren SJ. Urinary tract infections: epidemiology, mechanisms of infection and treatment options. Nature Reviews Microbiology. 2015;13(5):269-284. — doi:10.1038/nrmicro3432
- Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infectious Disease Clinics of North America. 2014;28(1):1-13. — doi:10.1016/j.idc.2013.09.003
- Williams G, Hahn D, Stephens JH, Craig JC, Hodson EM. Cranberries for preventing urinary tract infections. Cochrane Database of Systematic Reviews. 2023;(4):CD001321. — doi:10.1002/14651858.CD001321.pub6
- Howell AB, Botto H, Combescure C, et al. Dosage effect on uropathogenic Escherichia coli anti-adhesion activity in urine following consumption of cranberry powder. BMC Infectious Diseases. 2010;10:94. — doi:10.1186/1471-2334-10-94
- Eknoyan G, et al. The kidney and urinary tract in ancient Egyptian medicine PubMed: urinary tract in ancient Egyptian medicine
- Disorders of urination in the Hippocratic Collection — PubMed: PMID 15828260
- Uroscopy: history, Theophilus, and the matula PubMed: history of uroscopy
- History of urinary tract infection diagnosis and significant bacteriuria PubMed: history of UTI diagnosis
- Antibiotic resistance in uropathogenic E. coli and ESBL-producing strains PubMed: antibiotic resistance in UTI
External Authoritative Resources
- NIDDK (NIH) — Bladder Infection (Urinary Tract Infection) in Adults
- MedlinePlus — Urinary Tract Infections
- PubMed — History of urinary tract infection and Escherichia coli
Connections
- Urology
- Urinary Tract Infections
- Interstitial Cystitis (Painful Bladder Syndrome)
- Kidney Stones
- Benign Prostatic Hyperplasia
- Bladder Cancer
- All Conditions