Pulmonary Embolism: History and Discovery
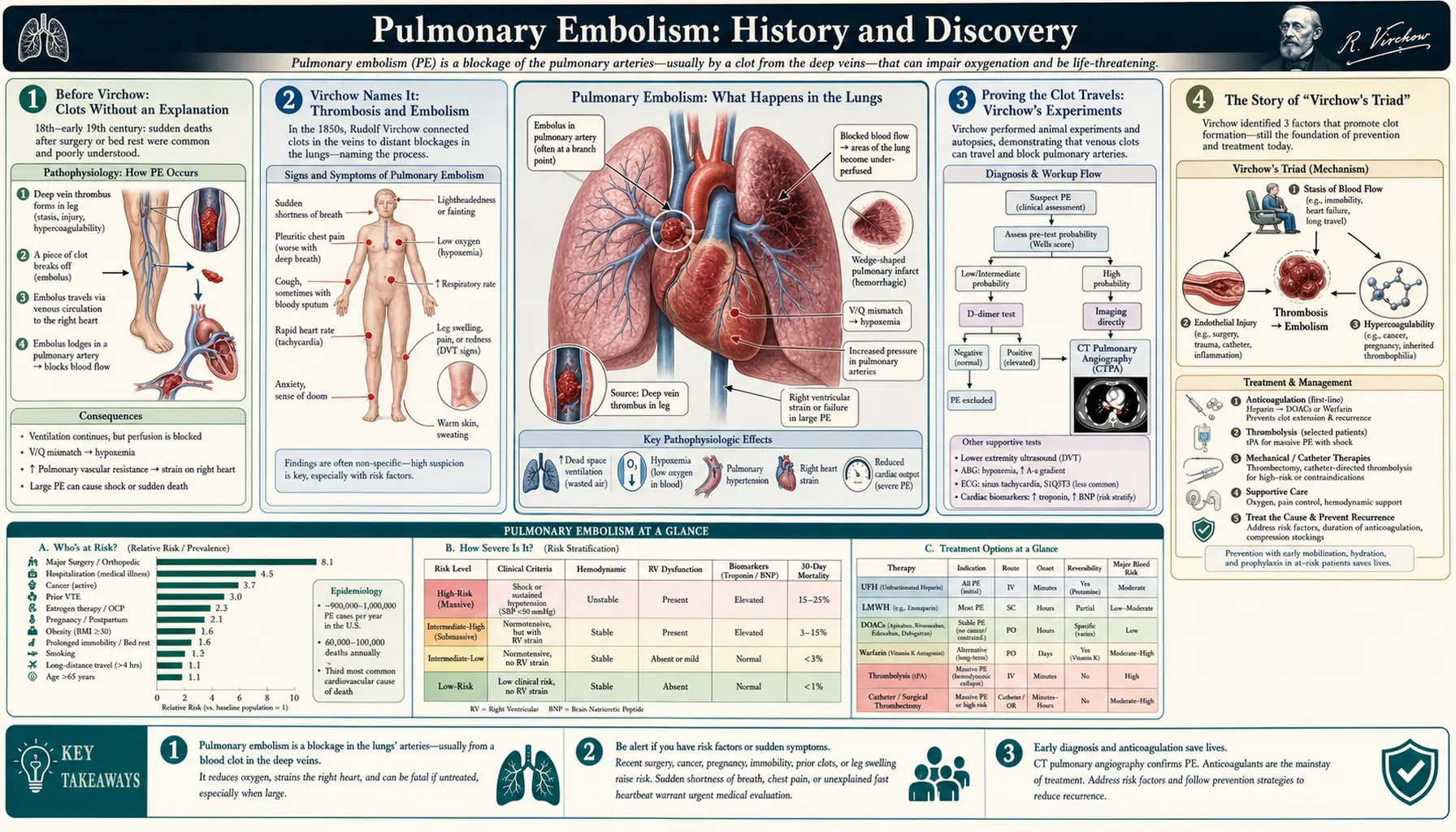
Pulmonary embolism (PE) is a blockage of an artery in the lung, almost always caused by a blood clot that has broken loose from a deep vein — usually in the leg or pelvis — and travelled through the heart into the lungs. Because the leg-vein clot (deep vein thrombosis, or DVT) and the lung blockage are two ends of the same disease, doctors group them together as venous thromboembolism. The figure at the center of this story is the German pathologist Rudolf Virchow, who in the 1840s and 1850s coined the very words “thrombosis” and “embolism” and proved by experiment that fragments of leg-vein clot are carried by the bloodstream and lodge in the lungs — overturning the older belief that the lung clots formed there on their own. For most of medical history PE was a deadly surprise found only at autopsy; the arrival of imaging, blood tests, anticoagulant drugs, and surgery turned it into a condition that can usually be diagnosed and treated while the patient is still alive. This page traces that long passage from mystery to manageable disease, and is careful to separate what was genuinely discovered, by whom, and when, from the popular shorthand that grew up around it.
Table of Contents
- Before Virchow: Clots Without an Explanation
- Virchow Names It: Thrombosis and Embolism
- Proving the Clot Travels: Virchow's Experiments
- The Story of “Virchow's Triad”
- The Autopsy Era: A Disease Found Too Late
- Seeing the Clot in the Living: Angiography to CTPA
- Heparin, Warfarin, and the Anticoagulant Revolution
- Surgery and Beyond: Trendelenburg, Filters, and Clot-Busters
- Legacy and Modern Understanding
- Research Papers and References
- Connections
- Featured Videos
Before Virchow: Clots Without an Explanation
For centuries physicians saw the effects of venous thrombosis and pulmonary embolism without understanding the connection between them. Swollen, painful legs — especially in women after childbirth, a condition once called phlegmasia alba dolens or “milk leg” — were recognized as a recurring affliction, but no one knew that the same process could kill suddenly by reaching the lungs. When sudden death was investigated after death, examiners sometimes found the great vessels of the lung plugged with clot, but the prevailing explanation was that the clot had grown there locally, as a product of inflamed veins.
That older framework went by the name phlebitis — literally inflammation of the veins — and it held that inflammation came first and caused the clot to form on the spot. Under this view a lung full of clot was simply phlebitis of the lung’s own vessels. The idea was reasonable for its time, but it was wrong in a way that mattered: if the clot grew where it was found, there was no reason to look at the legs, and no concept of a clot breaking loose and journeying through the circulation. The intellectual leap required was to imagine the clot as a traveller, and that leap is what Virchow supplied.
It is worth remembering how little of the modern picture existed in the early nineteenth century. There was no imaging, no blood test for clotting, and no drug that could safely thin the blood. Anatomy and the autopsy table were the only windows into the disease, and the meaning of what was seen there depended entirely on the theory the observer brought to it. Changing the theory, as it turned out, changed everything that followed.
Virchow Names It: Thrombosis and Embolism
Rudolf Virchow (1821–1902), working at the Charité hospital in Berlin early in his career, gave the field the vocabulary it still uses. In the mid-1840s — the terms are generally dated to 1846, a year after his first work on leukocytosis — he introduced the words “thrombosis” (from the Greek for a clot or clotting) for a clot forming within a vessel, and “embolism” (from the Greek embolos, a plug or stopper, originally something thrown in) for the lodging of a fragment carried by the blood into a distant vessel. Drawing this distinction — between a clot that forms in place and a clot that arrives from elsewhere — was the conceptual key to the whole disease.
These were not merely new labels for old ideas. By naming embolism, Virchow asserted that the material blocking a downstream vessel had come from somewhere upstream. The lung was the obvious place where such travelling clots would arrive, because all venous blood from the body passes through the right heart and then into the pulmonary arteries before reaching the lungs. A clot loosed from a leg vein, in this account, would be swept along this exact path and wedge in the lung — precisely what Virchow set out to demonstrate.
The naming also reframed phlebitis. Where the old doctrine put inflammation first and the clot second, Virchow’s work indicated that the clot generally came first and any inflammation followed it, rather than causing it. This reversal — quietly dismantling the “phlebitis” explanation of lung clots — is one of the reasons his contribution endured: he did not just add terms, he corrected the direction of cause and effect.
Proving the Clot Travels: Virchow's Experiments
Naming a phenomenon is not the same as proving it, and Virchow’s lasting authority rests on the fact that he supplied evidence. At the autopsy table he repeatedly noticed that thrombi in the lung and thrombi in the leg veins tended to occur together, and that the shapes often matched — a fragment in the lung could be fitted, like a broken piece, to the stump of a clot remaining in a vein, as though one had snapped off the other. This anatomical observation pointed directly to a clot that had detached and migrated.
He went further and tested the idea experimentally in animals, introducing foreign material or clot into the venous system and recovering it lodged in the pulmonary arteries, confirming that material from the veins is carried by the bloodstream into the lungs. His detailed exposition of this mechanism is associated with publications in the 1850s — commonly cited around 1856 for his account of venous thrombosis and embolism, with a vivid 1859 description of fragments detaching from a softening thrombus and being “driven into remote vessels.” The combination of matching autopsy specimens and reproducible experiments is what moved the travelling-clot idea from plausible hypothesis to established mechanism.
This is the heart of Virchow’s claim to the discovery of pulmonary embolism as a mechanism: he showed where the clot comes from and how it gets to the lung. It is important to be precise about the limit of that achievement, however. Virchow explained the process; he did not give physicians a way to diagnose it in a living patient, nor a way to treat it. Those two problems — seeing the clot in the living and dissolving or preventing it — would each take another century to solve, and they are the subjects of the sections that follow.
The Story of “Virchow's Triad”
Almost every medical student today learns “Virchow’s triad” — the three broad conditions that promote clot formation: sluggish or stagnant blood flow (stasis), a tendency of the blood itself to clot too readily (hypercoagulability), and injury to the inner lining of the vessel wall (endothelial or vessel injury). Together these explain why clots form in situations such as long immobility, surgery, cancer, pregnancy, and inherited clotting disorders. The framework is genuinely useful and genuinely important to understanding how DVT and PE begin.
Here, though, accuracy requires an honest correction of a near-universal myth. Virchow himself did not propose this triad. Historians who have examined his writings find that he never set out three factors as a unified list, and the modern grouping was assembled and attributed to him by later authors — the consensus three-factor formulation took shape decades after his death, and he only began to be routinely credited with “the triad” roughly a century after his work on venous thrombosis. The name is a posthumous honorific that compresses his ideas into a tidy teaching device he never wrote.
This page presents the triad as what the evidence shows it to be: a valid and valuable concept, named after Virchow rather than by him. Distinguishing the man’s real, demonstrated contributions — coining the terms, proving the embolic mechanism, correcting the phlebitis doctrine — from a later attribution is exactly the kind of care a history page owes its readers. The mechanism is sound; the attribution is a tradition, and it is fair to say so plainly.
The Autopsy Era: A Disease Found Too Late
For the better part of a century after Virchow explained the mechanism, pulmonary embolism remained chiefly a diagnosis of the dead. The classic clinical picture — sudden breathlessness, sharp chest pain that worsens with a breath, a racing heart, sometimes collapse — overlaps with heart attack, pneumonia, and many other emergencies, and there was no test that could single out a clot in the lung. Many fatal embolisms struck without warning, and a great number were first recognized only when the pathologist opened the chest and found the pulmonary arteries obstructed by clot. PE earned a reputation as a frequent and humbling “autopsy surprise.”
That reputation had real consequences. Because the disease could not be confirmed in life, it could not be treated in time, and prevention was guesswork. The link to leg-vein clots and to immobility — after surgery, after childbirth, during long confinement to bed — was increasingly suspected through careful clinical and pathological correlation, but suspicion is not diagnosis. The central problem of the early twentieth century was therefore not understanding PE in principle, which Virchow had largely settled, but catching it in practice, in a particular patient, while there was still time to act.
Two great advances were needed to break this deadlock, and they arrived from different directions in the twentieth century: a way to see the clot in a living person, and a class of drugs that could safely thin the blood to stop clots from forming and growing. The remainder of this history follows those two threads — diagnosis and treatment — as they converged to make PE a survivable disease.
Seeing the Clot in the Living: Angiography to CTPA
The first tools to reveal PE in a living patient were indirect or invasive. The chest X-ray and the electrocardiogram could hint at the diagnosis but could not confirm it. Pulmonary angiography — threading a catheter into the pulmonary arteries and injecting contrast dye to outline a blockage — gave a direct picture and long served as the reference standard, but it was invasive, demanding, and carried its own risks, so it was never a screening test. The ventilation/perfusion (V/Q) scan, a nuclear-medicine study that compares where air reaches the lungs with where blood reaches them, became a mainstay from the mid-twentieth century: a region that is ventilated but not perfused suggests a clot. The V/Q scan was less invasive but frequently returned “intermediate” results that left the question unsettled.
Two later developments transformed the everyday workup. The first was the D-dimer blood test, which measures a breakdown product of clot; its great value is its negative result — in a patient judged unlikely to have PE, a normal D-dimer can help safely rule the diagnosis out without imaging, though a raised level is non-specific and merely prompts further testing. The second, and decisive, advance was CT pulmonary angiography (CTPA). Built on helical (spiral) CT technology introduced clinically around 1990 and developed for the pulmonary arteries through the early-to-mid 1990s — with multidetector scanners arriving from 1998 — CTPA lets a contrast-enhanced scan show clot directly within the pulmonary arteries in seconds.
CTPA’s speed, availability, and accuracy made antemortem diagnosis of PE routine for the first time. As it spread, it largely displaced invasive pulmonary angiography and reduced reliance on the V/Q scan, which is now reserved mainly for patients who cannot receive iodinated contrast or should avoid radiation, such as some during pregnancy. Combined with structured clinical scoring and D-dimer, CTPA turned PE from a disease confirmed mainly at autopsy into one confirmed at the bedside. (One honest caveat: the ease of CTPA has also raised concern about over-diagnosis of very small clots of uncertain importance — a sign of how completely the diagnostic problem has reversed since Virchow’s day.)
Heparin, Warfarin, and the Anticoagulant Revolution
Diagnosis is only half the story; without a treatment, naming the clot in a living patient would change little. The cornerstone of PE treatment is anticoagulation — drugs that do not dissolve an existing clot directly but stop it from enlarging and prevent new clots, giving the body’s own systems time to break the clot down and letting the vessel heal. The first of these drugs was heparin, whose discovery is dated to 1916 from animal tissue; after considerable work to purify it for safe human use, heparin became a fast-acting injectable anticoagulant. Notably, the pioneering embolectomy surgeon Clarence Crafoord in Stockholm was among those who used heparin after surgery to help prevent venous thromboembolism, an early bridge between the surgical and drug approaches.
The second pillar was an oral anticoagulant for long-term use. Warfarin, a vitamin-K antagonist, was originally developed as a rodent poison and then adapted to medicine, entering clinical use in the 1950s; for decades the standard treatment of PE was rapid-acting heparin to begin with, overlapped with warfarin for months of ongoing protection. Warfarin was effective but demanding — it interacts with many foods and drugs and requires regular blood-test monitoring to keep its effect in a safe range.
The most recent chapter is the direct oral anticoagulants (DOACs), introduced in the twenty-first century, which block specific clotting factors and, in large trials, proved at least as effective as the old heparin-plus-warfarin approach for most patients while needing no routine monitoring and far fewer dietary restrictions. For this reason DOACs are now generally first-line for treating PE in suitable patients, with heparin and warfarin retained where they remain the better fit. The arc from a 1916 tissue extract to a tailored modern pill is, in practical terms, what made surviving a pulmonary embolism the expected outcome rather than a fortunate one.
Surgery and Beyond: Trendelenburg, Filters, and Clot-Busters
For the most catastrophic, life-threatening (“massive”) embolisms, where a large clot blocks the central pulmonary arteries and the patient is collapsing, physicians sought ways to remove or destroy the clot directly. The boldest early effort was surgical. In 1908 the German surgeon Friedrich Trendelenburg, professor of surgery at Leipzig, described an operation to open the pulmonary artery and physically extract the clot — the procedure that still bears his name, the Trendelenburg operation for pulmonary embolectomy. He worked the technique out in laboratory animals and attempted it in patients, but he did not achieve a surviving patient himself. The first successful Trendelenburg embolectomy was reported by his pupil Martin Kirschner in 1924, a milestone that proved a massive PE could, in principle, be survived through surgery.
Surgical embolectomy remained difficult and dangerous until the later advent of the heart-lung (cardiopulmonary bypass) machine made the operation far safer, and it is now reserved for selected severe cases or when clot-dissolving drugs are unsuitable or have failed. Alongside surgery, thrombolysis — powerful “clot-busting” drugs that actively dissolve clot — was developed for high-risk PE with dangerously low blood pressure, accepting a higher bleeding risk in exchange for rapidly relieving the obstruction. More recently, catheter-based techniques can deliver such therapy or mechanically remove clot through a thin tube, sparing some patients open surgery.
A separate line of defence is mechanical prevention with the inferior vena cava (IVC) filter — a small device placed in the large vein returning blood from the lower body, designed to catch clots breaking loose from the legs before they can reach the lungs. Filters are used mainly when anticoagulant drugs cannot be given safely (for example, in a patient with active bleeding) or when clots recur despite adequate anticoagulation, and many modern filters are retrievable once the danger has passed. Together these tools — embolectomy, thrombolysis, catheter therapies, and IVC filters — form the response to the most dangerous presentations of a disease that, a century ago, such patients rarely survived.
Legacy and Modern Understanding
The history of pulmonary embolism is a clear example of how naming and explaining a disease must come first, but is not enough on its own. Virchow’s nineteenth-century achievement — coining “thrombosis” and “embolism,” proving that leg-vein clots travel to the lungs, and discrediting the local-phlebitis theory — gave medicine the correct mental model. Yet for roughly a hundred years that correct model could not save many lives, because no one could reliably see the clot in a living patient or safely treat it. The twentieth and twenty-first centuries supplied the missing halves: imaging that culminated in CTPA, blood tests such as D-dimer, anticoagulant drugs from heparin to warfarin to the DOACs, and the surgical and mechanical options for the most severe cases.
Today PE and DVT are understood as two expressions of a single disorder, venous thromboembolism, and care reflects that unity: the same anticoagulant drugs treat both, and preventing DVT — through early mobility after surgery, compression, and preventive anticoagulation in high-risk patients — is recognized as the best way to prevent PE. The conditions Virchow’s name became attached to — stasis, hypercoagulability, and vessel injury — remain the working framework for identifying who is at risk, even though, as this page has been careful to note, the “triad” was formalized by others after him.
What was once a frequent and bewildering autopsy finding is now, for most patients, a diagnosable and treatable emergency with a good chance of recovery. That transformation took the combined labour of a pathologist with a microscope and a theory, surgeons willing to open the chest, chemists who tamed a poison into a medicine, and engineers who built scanners that see inside the lung in seconds. The story of PE is, in the end, a story of accumulated knowledge — each generation adding the piece the previous one lacked.
Research Papers and References
The references below combine peer-reviewed historical and clinical reviews with curated PubMed topic-search links into the literature on the discovery, diagnosis, and treatment of pulmonary embolism and venous thromboembolism. Where a stable identifier is available it is linked directly; the remaining entries open a relevant PubMed search. Each link opens in a new tab. Historical primary works by Virchow and Trendelenburg are named in the article as historical sources rather than as modern citations.
- Bagot CN, Arya R. Virchow and his triad: a question of attribution. British Journal of Haematology. 2008;143(2):180-190. — doi:10.1111/j.1365-2141.2008.07323.x
- Kumar DR, Hanlin E, Glurich I, Mazza JJ, Yale SH. Virchow’s contribution to the understanding of thrombosis and cellular biology. Clinical Medicine & Research. 2010;8(3-4):168-172. — doi:10.3121/cmr.2009.866
- Brinjikji W, Duffy S, et al. (historical review). Rudolf Virchow and the discovery of cerebral embolism. Stroke. — doi:10.1161/STROKEAHA.121.034443
- Dalen JE. Pulmonary embolism: what have we learned since Virchow? Natural history, pathophysiology, and diagnosis. Chest. 2002;122(4):1440-1456. — doi:10.1378/chest.122.4.1440
- Stein PD, Beemath A, et al. Multidetector computed tomography for acute pulmonary embolism (PIOPED II). New England Journal of Medicine. 2006;354(22):2317-2327. — doi:10.1056/NEJMoa052367
- Wittram C, Maher MM, Yoo AJ, et al. CT angiography of pulmonary embolism: diagnostic criteria and causes of misdiagnosis. RadioGraphics. 2004;24(5):1219-1238. — doi:10.1148/rg.245045008
- Friedrich Trendelenburg and the surgical approach to massive pulmonary embolism (historical review). Archives of Surgery. 1990. — PubMed 2205175
- The early history of anticoagulants and the discovery of heparin (1916) and warfarin — PubMed: history of heparin and warfarin
- Konstantinides SV, et al. Management of acute pulmonary embolism (ESC guidelines and reviews) — PubMed: acute PE management guidelines
- Direct oral anticoagulants (DOACs) for the treatment of venous thromboembolism — PubMed: DOACs for venous thromboembolism
- History of the ventilation/perfusion (V/Q) scan and pulmonary angiography in pulmonary embolism — PubMed: V/Q scan and pulmonary angiography
- D-dimer testing in the diagnosis and exclusion of pulmonary embolism — PubMed: D-dimer in PE diagnosis
- Surgical pulmonary embolectomy and the Trendelenburg operation: historical perspective — PubMed: surgical pulmonary embolectomy history
- Inferior vena cava (IVC) filters for the prevention of pulmonary embolism — PubMed: IVC filters for PE prevention
External Authoritative Resources
- NHLBI (NIH) — Pulmonary Embolism
- MedlinePlus — Pulmonary Embolism
- PubMed — History of pulmonary embolism
Connections
- Pulmonology
- Pulmonary Embolism (main page)
- Deep Vein Thrombosis
- Pulmonary Hypertension
- Disseminated Intravascular Coagulation
- Thrombocytopenia
- Atrial Fibrillation
- All Conditions