Acute Respiratory Distress Syndrome (ARDS): History and Discovery
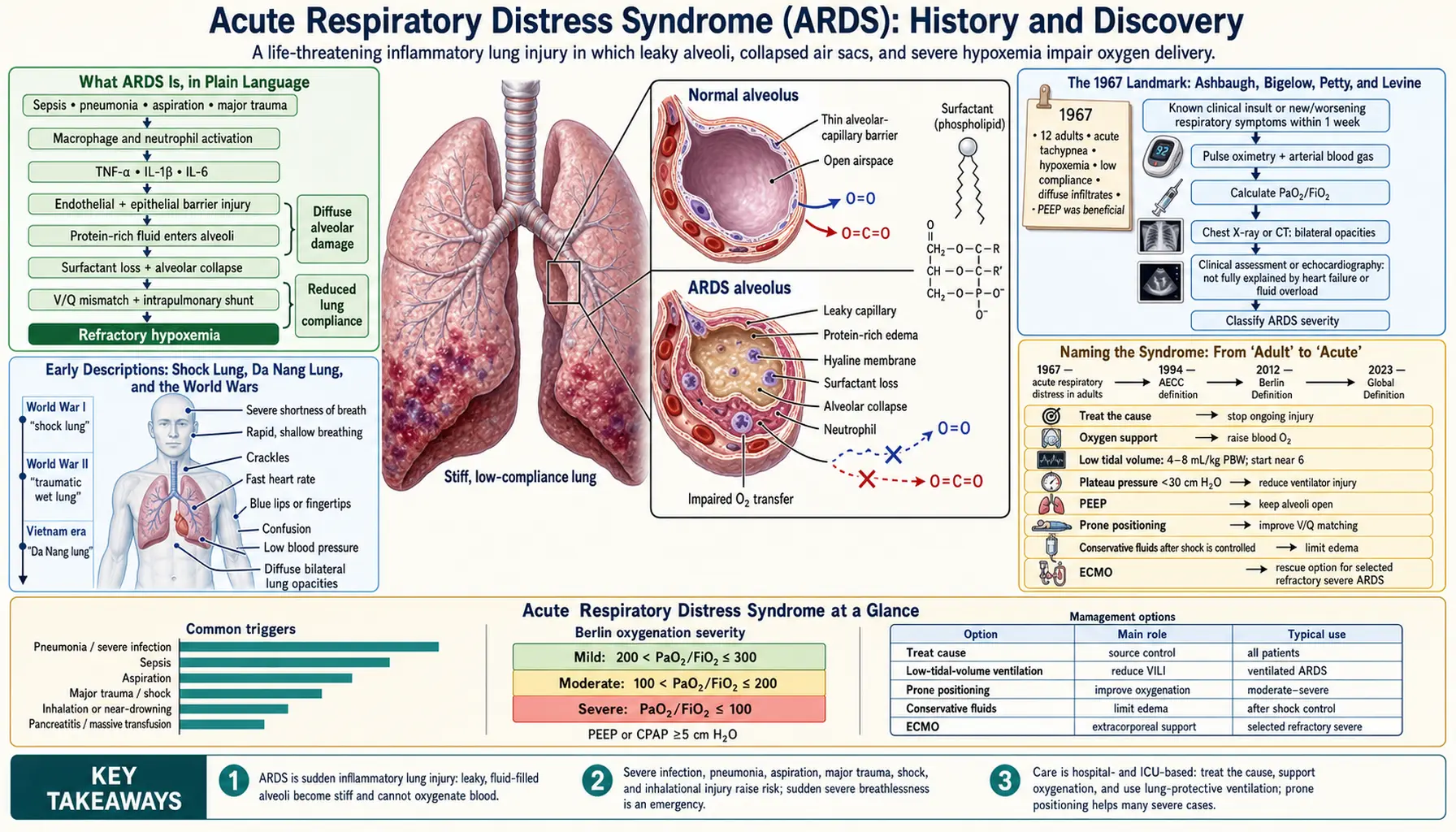
Acute Respiratory Distress Syndrome (ARDS) is a sudden, severe, and widespread injury to the lungs in which fluid floods the tiny air sacs, oxygen levels in the blood fall dangerously low, and a chest X-ray shows a near-total “white-out” of both lungs. Doctors had glimpsed this catastrophe for decades under a confusing patchwork of wartime and emergency-room nicknames — “shock lung,” “Da Nang lung,” “wet lung” — but it was first pulled together and described as a single recognizable syndrome in a landmark 1967 paper in The Lancet by David Ashbaugh, D. Boyd Bigelow, Thomas Petty, and Bernard Levine, who studied twelve patients whose lungs failed in the same striking way. This page traces ARDS from its scattered early descriptions, through the naming and renaming of the syndrome, to the consensus definitions (1994 and the 2012 Berlin Definition) and the treatment breakthroughs — above all lung-protective ventilation with low tidal volumes — that have saved many thousands of lives.
Table of Contents
- What ARDS Is, in Plain Language
- Early Descriptions: Shock Lung, Da Nang Lung, and the World Wars
- The 1967 Landmark: Ashbaugh, Bigelow, Petty, and Levine
- Naming the Syndrome: From “Adult” to “Acute”
- The 1994 American–European Consensus Definition
- The 2012 Berlin Definition
- The Great Treatment Breakthrough: Low Tidal Volumes (2000)
- Prone Positioning and the Modern Era
- Legacy and What the History Teaches
- Research Papers and References
- Connections
- Featured Videos
What ARDS Is, in Plain Language
Healthy lungs work like a delicate sponge full of hundreds of millions of microscopic air sacs called alveoli, each wrapped in tiny blood vessels. Oxygen crosses the paper-thin wall between air and blood with almost no resistance. In ARDS, that barrier breaks down: the lining of the alveoli and their capillaries becomes inflamed and leaky, and protein-rich fluid pours out of the bloodstream and into the air spaces. The lungs that should be light and airy become heavy, stiff, and waterlogged, which is why the old bedside name “wet lung” was so apt.
The consequences arrive fast and are easy to recognize once named. Breathing becomes rapid and labored, the blood oxygen level drops to dangerous lows (hypoxemia) that ordinary oxygen by mask cannot fix, and a chest X-ray shows both lungs clouded over — the dramatic “white-out” of widespread, fluffy infiltrates. Crucially, this flooding is not caused by a failing heart backing fluid up into the lungs; it is the lung tissue itself that is injured. ARDS is not a single disease with one cause but a final common pathway — a way the lungs respond to many different insults, including severe pneumonia, widespread infection (sepsis), major trauma, inhaling stomach contents, near-drowning, pancreatitis, and serious burns.
That “many roads to the same destination” quality is exactly why ARDS took so long to be recognized as one entity. For most of medical history, a patient whose lungs failed after a battlefield wound, a car crash, a blood transfusion, or a raging infection was given a different label depending on what had triggered the collapse. Seeing the underlying pattern — that all of these patients shared the same lung injury — was the conceptual leap that defines the history of ARDS.
Early Descriptions: Shock Lung, Da Nang Lung, and the World Wars
Long before ARDS had a name, military medicine kept colliding with it. In the trench warfare of the First World War, soldiers exposed to poison gases such as phosgene, and others who survived massive blood loss and shock from their wounds, sometimes developed a delayed and lethal flooding of the lungs hours after the initial injury — a pattern military physicians came to call “shock lung.” The lungs of these men, at autopsy, were heavy and sodden, quite unlike the lungs of someone who had simply bled to death. The syndrome reappeared among the wounded of the Second World War, again under the heading of shock lung or “traumatic wet lung,” tied to severe injury, transfusion, and resuscitation.
The most evocative of these names came out of the Vietnam War. Improved battlefield evacuation meant that gravely wounded soldiers who would once have died of blood loss were now surviving the initial trauma, only to deteriorate days later as their lungs filled with fluid — a complication that became known as “Da Nang lung,” after the major U.S. medical facility at Da Nang. The resemblance to the delayed lung failure of World War I gas casualties was so close that, by some historical accounts, military physicians initially wondered whether a chemical agent was responsible, before recognizing it as the lungs’ own response to shock, trauma, and massive resuscitation.
By the 1960s, then, the same fundamental injury was being seen and described under a scatter of names — shock lung, Da Nang lung, wet lung, “congestive atelectasis,” post-traumatic and post-transfusion lung — each tethered to its particular trigger. The pieces of the puzzle were all on the table; what was missing was someone to assemble them into a single syndrome and say plainly that these were all the same thing.
The 1967 Landmark: Ashbaugh, Bigelow, Petty, and Levine
That assembly happened in 1967. Writing in The Lancet, the American physicians David G. Ashbaugh, D. Boyd Bigelow, Thomas L. Petty, and Bernard E. Levine published a short paper with the deceptively simple title “Acute respiratory distress in adults.” In it they described twelve patients who, after a variety of different triggers, had all developed the same alarming picture: sudden rapid breathing, severe low blood oxygen that resisted ordinary oxygen therapy, stiff and poorly compliant lungs, and widespread infiltrates on chest X-ray. Importantly, this lung failure did not respond to the usual respiratory treatments of the day.
The paper’s genius was to recognize that the trigger did not matter to the lung: whatever the initial insult, the lungs responded in one stereotyped way. The authors also made an enduring practical observation — that adding positive end-expiratory pressure (PEEP), a technique of holding a little back-pressure in the airways at the end of each breath to keep the flooded air sacs from collapsing, helped combat the collapse (atelectasis) and improved oxygenation. PEEP remains a cornerstone of ARDS management to this day. Their description of the diffuse alveolar damage seen in these lungs laid the pathological foundation for everything that followed.
This 1967 report is universally credited as the first clear delineation of ARDS as a distinct clinical syndrome, and it is among the most cited papers in the history of critical care medicine. Thomas Petty in particular went on to champion the concept for decades, and the name he and his colleagues helped popularize — with one important later revision — is the one the world still uses. It is worth noting, as a point of accuracy, that the 1967 paper described and named a recognizable syndrome rather than discovering a previously unseen disease: the lung injury itself had been witnessed for half a century under other names, as described above.
Naming the Syndrome: From “Adult” to “Acute”
The acronym ARDS was not present in the 1967 title, which spoke simply of “acute respiratory distress in adults.” In the years that followed, the condition came to be widely called “Adult Respiratory Distress Syndrome” — deliberately echoing Infant (or Neonatal) Respiratory Distress Syndrome, the well-known lung condition of premature newborns. The parallel was attractive: both conditions involved stiff, poorly inflating lungs and dangerous low oxygen. The word adult served mainly to distinguish the grown-up syndrome from the newborn one.
Over time, however, the “adult” label proved to be misleading. It became clear that this same diffuse lung injury also strikes children, not adults alone. To keep the word “adult” in the name was therefore inaccurate and risked implying, wrongly, that young patients could not develop the syndrome. The fix was elegant: keep the familiar acronym ARDS but change what the first letter stands for. The condition was renamed “Acute Respiratory Distress Syndrome,” with acute — describing its sudden onset — replacing adult. The change was formalized by the consensus conference of 1994 discussed in the next section, which explicitly recommended “acute” over “adult” because the syndrome occurs in both adults and children.
This small change of a single word is one of the tidiest examples in medicine of a name being corrected to match reality without discarding decades of accumulated familiarity. Clinicians kept saying “ARDS” exactly as before; only the meaning behind the “A” quietly shifted from a statement about who gets the disease to a statement about how fast it strikes.
The 1994 American–European Consensus Definition
A clinical syndrome is only as useful as the definition that lets different doctors and researchers agree on who has it. Through the 1970s and 1980s, ARDS was diagnosed by judgment and rough criteria, which made it hard to compare studies or count cases reliably. To fix this, an expert panel convened by American and European critical-care societies published, in 1994, the American–European Consensus Conference (AECC) definition of ARDS, led by Gordon R. Bernard and colleagues.
The AECC offered the first widely adopted, standardized definition. It required an acute onset; bilateral infiltrates on the chest X-ray (the “white-out”); a low ratio of arterial oxygen to inspired oxygen (a PaO₂/FiO₂ ratio of 200 or below defined full ARDS, while a milder degree, 300 or below, was labeled “acute lung injury,” or ALI); and evidence that the fluid was not simply due to a failing heart (operationalized at the time as a pulmonary-artery wedge pressure of 18 mm Hg or less, or no clinical sign of left-sided heart failure). This same 1994 report is the document that cemented the “acute” rather than “adult” wording.
The AECC definition was a major step forward and powered nearly two decades of research, but experience exposed its weaknesses. The criteria for “acute” were vague, chest-X-ray reading proved unreliable between observers, the oxygenation cutoff ignored how much ventilator support a patient was receiving, and the wedge-pressure requirement became impractical as invasive monitoring fell out of favor. These limitations set the stage for a more rigorous revision.
The 2012 Berlin Definition
In 2012 a panel convened under the auspices of the European Society of Intensive Care Medicine, with the endorsement of the American Thoracic Society and the Society of Critical Care Medicine, published the Berlin Definition of ARDS in JAMA. Designed explicitly to be more reliable and easier to apply at the bedside, it remains the standard in use today and is the definition most clinicians mean when they speak of diagnosing ARDS.
The Berlin Definition’s most influential contribution was to grade ARDS by severity, based on how low the blood oxygen falls (the PaO₂/FiO₂ ratio) while the patient is on a standardized minimum amount of ventilator support (PEEP of at least 5 cm H₂O). It defined three tiers: mild (ratio above 200 up to 300), moderate (above 100 up to 200), and severe (100 or below). It also set a clearer time window — symptoms beginning within one week of a known insult — retained the requirement for bilateral opacities, and replaced the awkward wedge-pressure rule with the simpler stipulation that the lung failure not be fully explained by heart failure or fluid overload. The old separate category of “acute lung injury” was retired and folded in as “mild ARDS.”
Grading severity was not merely tidy bookkeeping: the severity tier tracks with the risk of dying and helps decide which aggressive therapies (such as prone positioning, discussed below) are warranted. The Berlin Definition thus turned a yes-or-no label into a graded scale that guides treatment. It is worth noting that definitions of ARDS continue to be discussed and refined by the critical-care community, including efforts to define the syndrome in children and in settings without advanced equipment; the Berlin Definition is the current consensus standard rather than a final word.
The Great Treatment Breakthrough: Low Tidal Volumes (2000)
For decades after 1967, doctors could recognize and define ARDS far better than they could treat it; the condition remained frequently fatal. The single most important treatment advance — and one of the great success stories of modern intensive care — arrived in 2000, when the U.S. ARDS Network (ARDSNet) published the results of a large randomized trial, often called the ARMA trial, in The New England Journal of Medicine. It changed how mechanical ventilators are set for these patients all over the world.
The insight behind the trial was counter-intuitive. The natural instinct, faced with lungs that cannot oxygenate the blood, is to push more air in with each breath. But researchers had come to suspect that large breaths were actually injuring the fragile, inflamed lung further — over-stretching the few healthy air sacs and worsening the damage, a phenomenon called ventilator-induced lung injury. The trial tested lung-protective ventilation: deliberately small breaths (a low tidal volume of about 6 milliliters per kilogram of predicted body weight, with limits on airway pressure) versus the traditional larger breaths of around 12 mL/kg.
The result was decisive enough that the trial was stopped early: the gentler, smaller-breath strategy significantly reduced deaths (mortality fell to roughly 31% in the low-volume group, compared with about 40% with traditional volumes) and got patients off the ventilator sooner. In other words, ventilating the lungs more gently — doing less — saved lives. Lung-protective ventilation with low tidal volumes became, and remains, the foundation of ARDS care and is one of the most firmly established life-saving interventions in all of critical-care medicine. It is the central reason that surviving ARDS became far more likely after the year 2000.
Prone Positioning and the Modern Era
A second major advance concerned not the ventilator settings but the patient’s position. Clinicians had observed for years that turning a severely affected ARDS patient onto their stomach — prone positioning, or “proning” — often improved oxygen levels, because it helps air and blood flow reach lung regions that are crushed and collapsed when the patient lies on their back. For a long time it was unclear whether this temporary improvement in numbers actually helped patients survive.
The question was settled in 2013 by the PROSEVA trial, led by Claude Guérin and colleagues and published in The New England Journal of Medicine. In patients with severe ARDS, applying prolonged prone-positioning sessions early — on the order of sixteen hours a day — produced a striking reduction in death compared with keeping patients on their backs. Proning, like low-tidal-volume ventilation, thus moved from a plausible bedside trick to an evidence-based, life-saving therapy reserved for the sickest patients, exactly the group identified as “severe” by the Berlin Definition.
Together, the 1967 description, the careful 1994 and 2012 definitions, and the treatment trials of 2000 and 2013 form a coherent arc: first recognize the syndrome, then define and grade it precisely, then prove which treatments actually save lives. Other supportive measures — conservative fluid management, careful sedation, and, for the most extreme cases, extracorporeal membrane oxygenation (ECMO, an artificial lung that oxygenates the blood outside the body) — round out the modern toolkit, but lung-protective ventilation and prone positioning remain the two interventions most clearly shown to reduce mortality.
Legacy and What the History Teaches
The history of ARDS is, more than anything, a story about seeing a pattern. For fifty years the same diffuse lung injury was witnessed on battlefields and in emergency rooms under a dozen different names, each tied to whatever had triggered it. The lasting achievement of the 1967 Lancet paper was to recognize that the lungs respond to many different catastrophes in one stereotyped way, and to give that pattern a single name — an idea so useful it reorganized an entire field of medicine.
It is also a story about the discipline of definitions. A syndrome cannot be studied, counted, or compared across hospitals until experts agree on exactly what it is, and the steady refinement from the loose criteria of the 1980s, through the 1994 American–European consensus, to the graded 2012 Berlin Definition shows medicine improving its own vocabulary so that research can build cumulatively. The quiet correction of “adult” to “acute” belongs to the same impulse: keep what works, fix what is wrong.
Finally, and most hopefully, the ARDS story shows that careful science changes outcomes. The condition was once almost a death sentence; the demonstration in 2000 that gentler ventilation saves lives, and in 2013 that turning the sickest patients onto their stomachs saves more, turned a frequently fatal syndrome into one that many people now survive. For patients and families facing ARDS today, that history carries a real and grounded message: the modern treatment of this terrifying illness rests on hard-won evidence, and survival has improved dramatically because of it. The companion ARDS overview page covers causes, symptoms, diagnosis, and current treatment in practical detail.
Research Papers and References
The references below combine the landmark primary papers that define the history of ARDS with curated PubMed topic-search links into the broader historical and clinical literature. Direct journal links are given where a stable DOI or PubMed record is available; each link opens in a new tab. Readers should remember that this is an educational history page, not medical advice, and that ARDS is a life-threatening emergency managed by critical-care specialists.
- Ashbaugh DG, Bigelow DB, Petty TL, Levine BE. Acute respiratory distress in adults. The Lancet. 1967;2(7511):319-323. (The landmark first description of the syndrome in 12 patients.) — doi:10.1016/S0140-6736(67)90168-7
- Bernard GR, Artigas A, Brigham KL, et al. The American-European Consensus Conference on ARDS. Definitions, mechanisms, relevant outcomes, and clinical trial coordination. American Journal of Respiratory and Critical Care Medicine. 1994;149(3 Pt 1):818-824. (The 1994 AECC definition; formalized “acute” in place of “adult.”) — Search PubMed
- The Acute Respiratory Distress Syndrome Network (ARDSNet). Ventilation with lower tidal volumes as compared with traditional tidal volumes for acute lung injury and the acute respiratory distress syndrome. New England Journal of Medicine. 2000;342(18):1301-1308. (The ARMA trial; low-tidal-volume lung-protective ventilation.) — doi:10.1056/NEJM200005043421801
- The ARDS Definition Task Force. Acute respiratory distress syndrome: the Berlin Definition. JAMA. 2012;307(23):2526-2533. (The current consensus definition with mild/moderate/severe grading.) — PMID: 22797452
- Guérin C, Reignier J, Richard JC, et al. Prone positioning in severe acute respiratory distress syndrome. New England Journal of Medicine. 2013;368(23):2159-2168. (The PROSEVA trial.) — doi:10.1056/NEJMoa1214103
- History of ARDS and the evolution of its definitions PubMed: history and evolution of the ARDS definition
- Shock lung, traumatic wet lung, and the wartime origins of the ARDS concept PubMed: shock lung and the wartime history of ARDS
- From “adult” to “acute” — the renaming of the respiratory distress syndrome PubMed: “adult” vs “acute” respiratory distress syndrome terminology
- Diffuse alveolar damage — the pathology underlying ARDS PubMed: diffuse alveolar damage in ARDS
- Positive end-expiratory pressure (PEEP) in ARDS — history and physiology PubMed: PEEP in acute respiratory distress syndrome
- Ventilator-induced lung injury and the rationale for lung-protective ventilation PubMed: ventilator-induced lung injury and lung-protective ventilation
- Prone positioning in ARDS — mechanisms and clinical evidence PubMed: prone positioning in ARDS
- Pediatric acute respiratory distress syndrome (PARDS) — defining ARDS in children PubMed: pediatric ARDS definition
- Epidemiology and outcomes of ARDS — how survival has changed over time PubMed: ARDS epidemiology and outcomes
External Authoritative Resources
- National Heart, Lung, and Blood Institute (NHLBI) — ARDS
- MedlinePlus — Acute Respiratory Distress Syndrome
- PubMed — All research on acute respiratory distress syndrome
Connections
- Pulmonology
- Acute Respiratory Distress Syndrome (overview)
- Pneumonia
- Sepsis
- Pulmonary Embolism
- Interstitial Lung Disease
- All Conditions