Cellulitis: History and Discovery
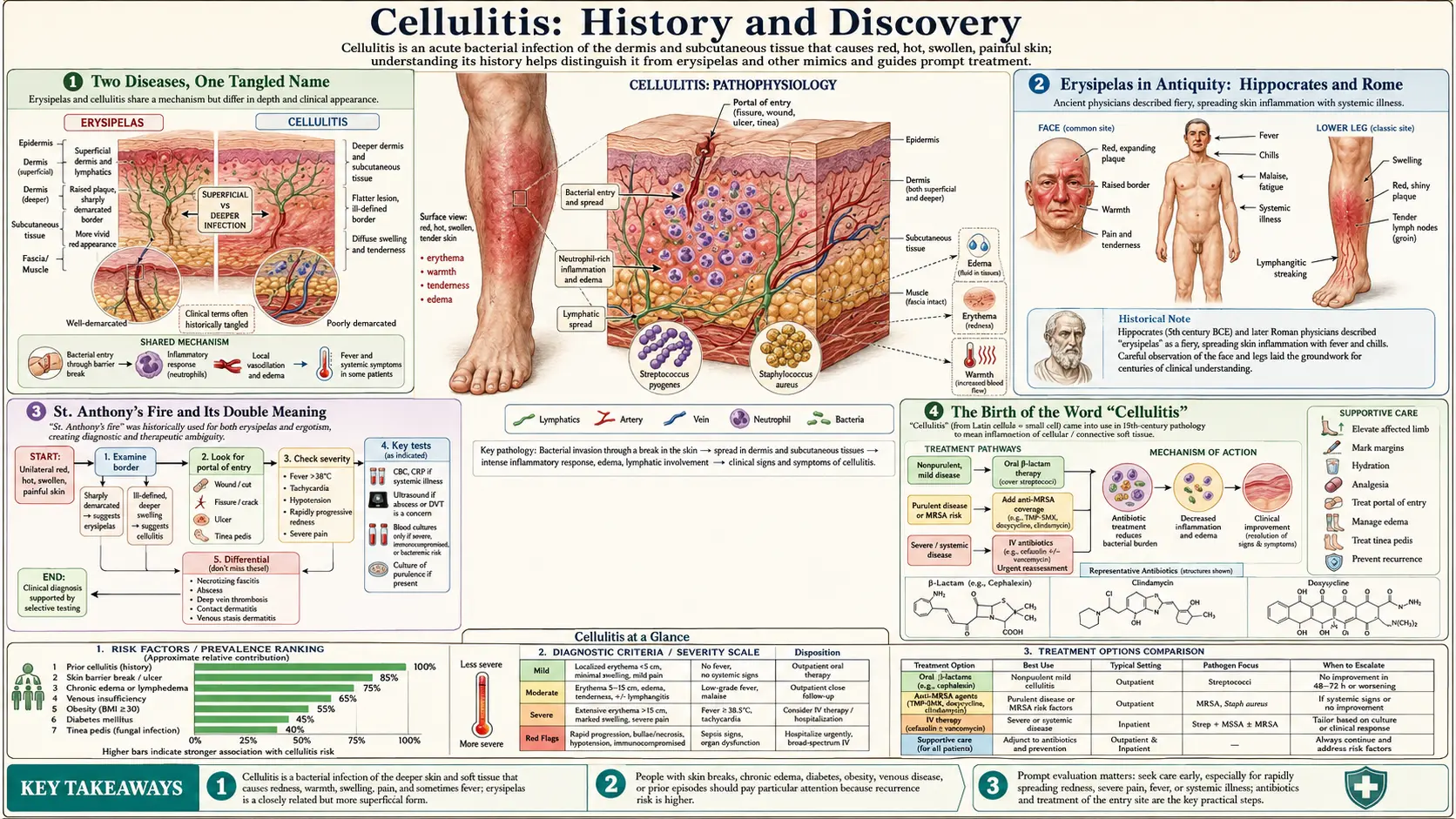
Cellulitis — a bacterial infection of the skin and the soft tissue beneath it — has one of the longest and most tangled histories in medicine, because for most of that history it had no name of its own. Its story is braided together with erysipelas, the spreading, fiery-red skin infection that physicians have described since antiquity. The Greek physician Hippocrates wrote of erysipelas (literally “red skin”) in the fourth century BCE; medieval Europeans called the burning rash St. Anthony’s fire — a name they also, confusingly, gave to ergotism, a poisoning from a fungus on rye. The word “cellulitis” itself is a nineteenth-century invention, coined when anatomists began to speak of inflammation of the body’s “cellular” (connective) tissue. Only with the rise of germ theory did the true cause emerge: chains of bacteria — chiefly Streptococcus and Staphylococcus. Theodor Billroth coined the word Streptococcus in 1874; Friedrich Fehleisen pinned that organism to erysipelas in 1883. Before antibiotics these infections could be lethal; sulfa drugs in the 1930s and penicillin in the 1940s transformed a once-dreaded disease into a routinely curable one. This page traces that long road, naming names and dates carefully, and flags hypothesis as hypothesis.
Table of Contents
- Two Diseases, One Tangled Name
- Erysipelas in Antiquity: Hippocrates and Rome
- St. Anthony’s Fire and Its Double Meaning
- The Birth of the Word “Cellulitis”
- Germ Theory and the Naming of Streptococcus
- Fehleisen, Koch’s Postulates, and the Cause Confirmed
- A Strange Detour: Erysipelas and Coley’s Toxins
- Sulfa, Penicillin, and the End of a Killer
- The Modern Distinction and Its Limits
- Research Papers and References
- Connections
- Featured Videos
Two Diseases, One Tangled Name
To understand the history of cellulitis you must first accept a frustrating fact: for more than two thousand years, the conditions we now separate as erysipelas and cellulitis were not clearly distinguished, and the words used for them slid around freely. Both are infections that make a patch of skin hot, red, swollen, and painful, and both can spread alarmingly fast. To an ancient or medieval observer they looked like one fearsome thing — a fire under the skin. The careful modern split — erysipelas as a superficial infection of the upper dermis with sharply raised, well-defined borders, and cellulitis as a deeper infection reaching the lower dermis and the subcutaneous fat, with edges that fade gradually into normal skin — is a relatively recent refinement.
This matters for honest history because it is tempting, but wrong, to say that any single physician “discovered cellulitis.” No one did. What actually happened is a long, gradual process: an ancient clinical picture (erysipelas) was described and re-described for centuries; a new anatomical word (“cellulitis”) was minted in the 1800s for inflammation of the connective tissue; and, separately, the microbial cause of these skin infections was uncovered by the microbiologists of the germ-theory era. Three different threads — the clinical picture, the word, and the cause — were woven together only in the late nineteenth and twentieth centuries.
Throughout this page, then, we treat “the history of cellulitis” as inseparable from the history of erysipelas, while being explicit about which thread we are following at any moment. Where a claim is a historical interpretation rather than a documented fact, it is labelled as such.
Erysipelas in Antiquity: Hippocrates and Rome
The clinical story begins in classical Greece. The word erysipelas appears in the Hippocratic Corpus, the body of medical writings associated with Hippocrates of Cos (roughly 460–370 BCE). The term is built from two Greek roots commonly given as erythros (“red”) and pella (“skin”) — a plain, descriptive name for a red skin disease. Streptococcal skin infection, in other words, has been recognized as a distinct clinical entity since at least the fourth century BCE, making it one of the oldest named infectious diseases in the Western record.
Importantly, the Hippocratic writers already grasped something we still teach: that this red, spreading inflammation often followed an injury. They distinguished a traumatic erysipelas, arising in and around wounds, from skin eruptions with no obvious external cause. Because the ancient term was applied broadly, much of what the Hippocratic authors called erysipelas would, by modern definitions, include what we now call cellulitis — another reason the two histories cannot be cleanly separated. (Dioscorides, Galen, and other classical authors are named here as historical primary sources rather than modern citations.)
Roman medicine carried the same picture forward, often under the Latin label ignis sacer, “sacred fire” or “holy fire” — a phrase used in antiquity for several conditions that produced a burning sensation in the skin, erysipelas among them. That older “fire” imagery would re-emerge, transformed, in the medieval name for the disease.
St. Anthony’s Fire and Its Double Meaning
In the European Middle Ages, the burning red skin disease acquired a vivid new name: St. Anthony’s fire (also written “Saint Anthony’s fire”). The name is generally traced to the Order of St. Anthony (the Antonines), a hospital brotherhood founded in France in the late eleventh century that became famous for nursing sufferers of a devastating epidemic affliction. The “Anthony” in question is usually taken to be St. Anthony the Great, the third-century Egyptian hermit and founder of Christian monasticism, whose relics the order venerated.
Here lies one of the most important — and most honestly confusing — points in this whole history. “St. Anthony’s fire” has a double meaning. The name was applied to two completely different diseases:
First, it was used for erysipelas, the streptococcal skin infection that is this page’s subject — an understandable label for a fiery red rash. Second, and arguably more often in the medical-historical literature, it referred to ergotism: a poisoning, not an infection at all, caused by eating rye and other grains contaminated with the fungus Claviceps purpurea (ergot). Ergot’s alkaloids constrict blood vessels and can produce searing burning pain, gangrene of the limbs, and convulsions. Medieval ergotism epidemics killed thousands at a stroke — an outbreak in Sologne, France, in 1778 is reported to have claimed on the order of eight thousand lives. Several authorities argue that, strictly, “St. Anthony’s fire” is best understood as an eponym for ergotism rather than erysipelas, even though popular and clinical usage has long applied it to both.
For a reader of a cellulitis history page, the takeaway is simply to be careful: when you encounter “St. Anthony’s fire” in an old text, it may mean the streptococcal skin infection (erysipelas/cellulitis) or the rye-fungus poisoning (ergotism). The shared element is only the symptom — a burning fire in the flesh — not the underlying disease. This page flags the ambiguity rather than pretending the old name mapped neatly onto cellulitis.
The Birth of the Word “Cellulitis”
The word “cellulitis” is much younger than the disease it names. It is a nineteenth-century coinage, assembled in the standard medical fashion from the Latin cellula — the diminutive of cella, “a small chamber” or “cell” — plus the suffix -itis, denoting inflammation. Literally, then, “cellulitis” means inflammation of the cellular tissue. The “cellular tissue” here is not the cell of modern cell biology but the older anatomical sense: the loose cellular (areolar, connective) tissue that fills the spaces beneath the skin and between the body’s structures. Nineteenth-century anatomists pictured this layer as a network of tiny compartments or cells, and inflammation spreading through it was “cellulitis.”
According to the Oxford English Dictionary, the earliest evidence for the noun cellulitis dates to the 1840s, with a cited use from 1849 in Guy’s Hospital Reports. The term thus entered medical English squarely in the mid-Victorian period, decades before anyone understood that bacteria caused the inflammation it described. At first it was a purely anatomical and clinical label — a description of where the inflammation was (in the cellular tissue) and that it was inflamed — with no implication about microbial cause.
This sequence is worth stressing because it overturns a natural assumption. People often imagine that a disease is first “discovered,” then named, then explained. With cellulitis the order was different: the clinical picture was ancient (erysipelas), the word arrived in the 1840s as an anatomical description, and the cause was established later still. The name “cellulitis” was waiting, fully formed, for germ theory to fill it with meaning.
Germ Theory and the Naming of Streptococcus
The nineteenth century’s great revolution — the germ theory of disease — finally connected the ancient red rash and the new anatomical word to a physical cause. The French chemist Louis Pasteur (1822–1895) demonstrated that microorganisms drive fermentation and putrefaction and championed the idea that specific microbes cause specific diseases; the German physician Robert Koch (1843–1910) supplied the rigorous experimental framework — later codified as Koch’s postulates — for proving that a particular organism causes a particular illness. Pasteur himself worked on streptococci, isolating chain-forming bacteria from cases of puerperal (childbed) fever and other infections.
The organism at the heart of cellulitis and erysipelas got its enduring name in this era. In 1874, the eminent Austrian surgeon Theodor Billroth (1829–1894), studying wound infections and erysipelas, described tiny round bacteria arranged in chains and coined the word Streptococcus — from the Greek streptos, “twisted” or “a chain,” and kokkos, “berry” or “grain.” The name pictures the bacterium exactly: beads on a string, a chain of berries. Billroth’s coinage gave microbiology a word it has used ever since.
The naming was refined over the following decade. In 1884, the German physician Friedrich Julius Rosenbach applied the species name Streptococcus pyogenes (“pus-forming”) to the chain-forming organisms he cultured from suppurating wounds — the same group A streptococcus we now recognize as the leading cause of erysipelas and a frequent cause of cellulitis. With Billroth’s genus and Rosenbach’s species, the bacterium finally had a stable scientific identity.
Fehleisen, Koch’s Postulates, and the Cause Confirmed
Naming a chain-forming bacterium found in infected wounds is not the same as proving it causes a specific disease. That decisive step, for erysipelas, belongs to the German surgeon Friedrich Fehleisen (1854–1924). In 1883, Fehleisen isolated streptococci in pure culture from the lesions of erysipelas patients and then showed that inoculating these cultures could reproduce typical erysipelas — thereby satisfying the chain of evidence demanded by Koch’s postulates and establishing the streptococcus as the cause of the disease. Fehleisen’s 1883 work is the single most important landmark in pinning down the microbial cause of erysipelas, and by extension of much of what we call streptococcal cellulitis.
It is worth being precise about what Fehleisen demonstrated and what he did not. He established the cause of erysipelas specifically — the sharply demarcated, superficial form. The recognition that deeper soft-tissue infection (cellulitis in the modern sense) is frequently caused by the same streptococci, and also by Staphylococcus species, came together gradually as bacteriological wound culture matured in the late nineteenth and early twentieth centuries. The historical rule of thumb that hardened over the following decades — streptococci behind the spreading, superficial erysipelas; staphylococci more often behind localized, deeper, pus-forming infection — is a simplification, but it captures how clinicians of the era learned to read these infections.
By the close of the nineteenth century, then, all three threads had finally been joined. The ancient clinical picture (erysipelas, described since Hippocrates), the Victorian anatomical word (“cellulitis,” coined in the 1840s), and the microbial cause (streptococci named by Billroth in 1874, confirmed in erysipelas by Fehleisen in 1883) were now understood as facets of one phenomenon: bacterial infection of the skin and its underlying tissue.
A Strange Detour: Erysipelas and Coley’s Toxins
One of the most remarkable episodes in this history is a genuine medical curiosity, and it must be told carefully as hypothesis, not established cure. In the late nineteenth century the American bone surgeon William B. Coley (1862–1936), working at what became Memorial Hospital in New York, was haunted by the death of a young cancer patient in 1891. Searching hospital records, he found documented cases in which a malignant tumor had shrunk or vanished after the patient happened to develop a severe erysipelas infection — the fever and inflammation seeming, somehow, to attack the cancer.
Coley formed a hypothesis: that the bacterial infection had roused the body’s defenses to turn on the tumor. Beginning in 1893 he deliberately tried to harness this effect, ultimately developing a preparation of killed bacteria — Streptococcus pyogenes combined with Serratia marcescens — that became known as Coley’s toxins. He treated hundreds of cancer patients with it over his career and reported some striking regressions.
Modern medicine regards Coley as a prescient, if controversial, forerunner of cancer immunotherapy — the idea that the immune system can be mobilized against tumors. But it is essential to be clear and honest: Coley’s toxins were never a proven, reliable cancer cure; his results were uncontrolled by today’s standards, inconsistent, and eventually eclipsed by radiation and chemotherapy. The story belongs here only because it shows how central erysipelas once was to medical thinking — so feared, yet so powerful in its effects, that a surgeon tried to turn the infection itself into a treatment. The underlying immunological insight was real; the specific therapy remained a hypothesis that history never fully validated.
Sulfa, Penicillin, and the End of a Killer
For all the progress in understanding cellulitis and erysipelas, physicians of the early twentieth century still had almost nothing to cure them. Before effective antibacterial drugs, a spreading streptococcal skin infection was a serious, sometimes fatal, illness: it could invade the bloodstream and cause overwhelming sepsis, and surgical wards lived in dread of erysipelas sweeping from patient to patient. Care meant rest, wound dressing, and hope.
The first true turning point came from the sulfonamides. The red azo dye Prontosil was synthesized in 1932 by the chemists Josef Klarer and Fritz Mietzsch, and the German pathologist Gerhard Domagk (1895–1964) showed that it cured streptococcal infections in mice; he published these findings in 1935, opening the antibacterial era and later earning a Nobel Prize. Erysipelas was among the very first human diseases on which the new sulfa drugs were tried — pioneering controlled clinical trials of sulfonamides for erysipelas were carried out in Glasgow beginning in the mid-1930s — and for the first time the spreading infection could be reliably halted.
The second, even greater, transformation was penicillin. Discovered as a mold product by Alexander Fleming in 1928 and developed into a usable drug by Howard Florey, Ernst Chain, and their Oxford team around 1940–1941, penicillin proved devastatingly effective against streptococci and many staphylococci. From the 1940s onward, erysipelas and cellulitis — diseases that had frightened physicians since Hippocrates — became, in most cases, straightforwardly treatable. Penicillin and its descendants remain a backbone of cellulitis therapy to this day, though the later spread of antibiotic-resistant organisms such as MRSA (methicillin-resistant Staphylococcus aureus) has complicated treatment and returned a measure of caution to a once-conquered disease.
The Modern Distinction and Its Limits
Only in the twentieth century did the now-standard distinction between erysipelas and cellulitis become a firm clinical convention. The modern teaching draws the line by depth and definition: erysipelas is the more superficial infection, involving the upper dermis and the superficial lymphatic vessels, and it classically presents as a brightly red, raised plaque with sharply demarcated, well-defined borders — you can almost trace its edge with a pen. Cellulitis reaches deeper, into the lower dermis and the subcutaneous fat, and its margins are indistinct, fading gradually into surrounding skin. Erysipelas is attributed chiefly to streptococci; cellulitis may be caused by streptococci, by Staphylococcus aureus, or by other organisms.
Yet even this tidy split has real limits, and honest sources acknowledge them. In everyday practice the two overlap heavily, the boundary between “upper” and “lower” dermis is not something the eye can measure, and many clinicians and guidelines treat erysipelas as essentially a form of, or a near synonym for, superficial cellulitis. The old habit of inferring the germ from the appearance — streptococcal if sharply edged, staphylococcal if not — is a useful heuristic rather than a reliable rule, since cultures are often negative and the clinical pictures blur into one another.
So the modern distinction is best seen as the last chapter of a very long story rather than its tidy resolution. From Hippocrates’ “red skin,” through the medieval fires of St. Anthony, the Victorian coining of “cellulitis,” and the germ-theory unmasking of the streptococcus, medicine slowly pulled one ancient, fearsome phenomenon into focus — naming it, explaining it, and at last learning to cure it. That the names still overlap a little is a fitting reminder that the history of cellulitis is, and always has been, the history of erysipelas told twice. For the present-day clinical picture, diagnosis, and treatment, see the main Cellulitis page.
Research Papers and References
The references below combine peer-reviewed reviews and historical scholarship on erysipelas, cellulitis, and the streptococcus with curated PubMed topic-search links into the primary literature. Ancient and early-modern authors (Hippocrates, Dioscorides, Galen) are named in the article as historical primary sources rather than as modern citations. Each external link opens in a new tab.
- Bonnetblanc JM, Bedane C. Erysipelas: recognition and management. American Journal of Clinical Dermatology. 2003;4(3):157-163. — doi:10.2165/00128071-200304030-00002
- Stevens DL, Bryant AE. Impetigo, Erysipelas and Cellulitis. In: Streptococcus pyogenes: Basic Biology to Clinical Manifestations. University of Oklahoma Health Sciences Center; 2016. — NCBI Bookshelf: Impetigo, Erysipelas and Cellulitis
- Ferretti J, Köhler W. History of Streptococcal Research. In: Streptococcus pyogenes: Basic Biology to Clinical Manifestations. 2016. — NCBI Bookshelf: History of Streptococcal Research
- Etymologia: Streptococcus. Emerging Infectious Diseases (CDC). 2016;22(11):1947. — doi:10.3201/eid2211.ET2211
- Bryan CS, et al. St. Anthony’s fire: an eponym for ergotism, not erysipelas. (PubMed citation) — PubMed 7604780
- Tóth B, et al. Pioneering controlled trials of treatments for erysipelas and pneumonia in Glasgow, 1936–1947. Journal of the Royal Society of Medicine. 2019. — PMC6613273
- McCarthy EM, et al. William Coley and erysipelas-induced tumour regression: the origins of cancer immunotherapy. — PubMed: Coley’s toxins, erysipelas and tumour regression
- Fehleisen F — streptococci as the cause of erysipelas (1883); Koch’s postulates in erysipelas. — PubMed: Fehleisen, erysipelas and streptococcus
- Billroth, Rosenbach, and the naming of Streptococcus and Streptococcus pyogenes. — PubMed: history of Streptococcus pyogenes nomenclature
- Domagk G, Prontosil, and the discovery of the sulfonamides. — PubMed: Domagk, Prontosil and the sulfonamides
- Penicillin: Fleming, Florey, Chain and the development of the first antibiotic. — PubMed: history of penicillin
- Hippocrates, the Hippocratic Corpus, and infectious disease in classical antiquity. — PubMed: Hippocrates and infectious disease
- Ergotism, Claviceps purpurea, and St. Anthony’s fire in medieval Europe. — PubMed: ergotism and St. Anthony’s fire
- Erysipelas and cellulitis: clinical distinction, microbiology, and management (review). — PubMed: erysipelas vs cellulitis
External Authoritative Resources
- StatPearls (NCBI Bookshelf) — Cellulitis
- Oxford English Dictionary — “cellulitis” (etymology & earliest use)
- PubMed — history of cellulitis and erysipelas
Connections
- Infectious Disease
- Cellulitis
- All Conditions
- Sepsis
- Fungal Infections
- Staphylococcus aureus
- Erysipelas — the superficial streptococcal infection whose history this page shares.