Gallbladder Disease: History and Discovery
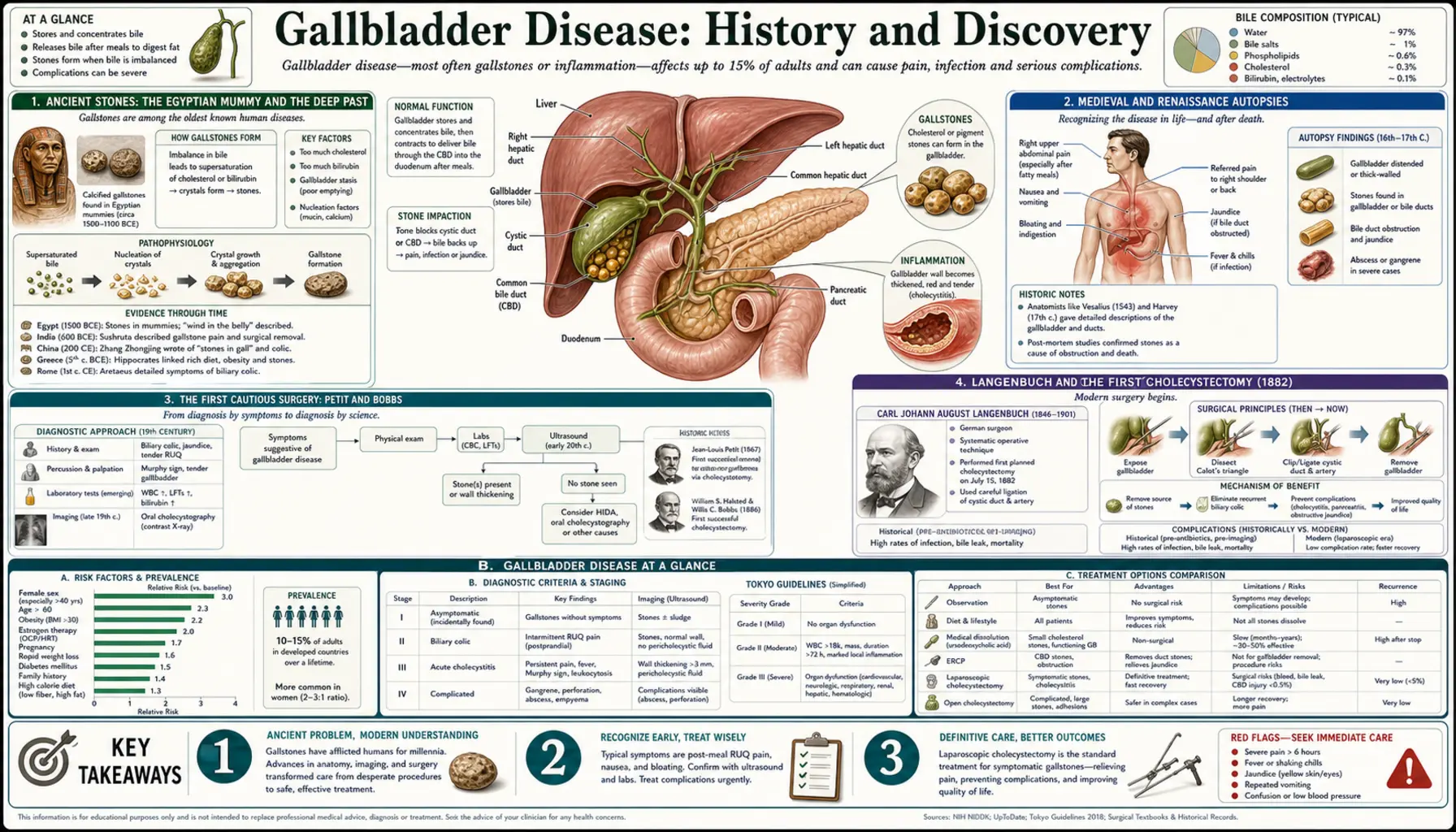
Gallstones are one of the oldest documented human diseases. Hard stones have been recovered from the embalmed body of an ancient Egyptian priestess, sat unnamed in medieval and Renaissance autopsy notebooks, and waited centuries before anyone dared to operate on the small green organ that made them. This page traces that long arc — from stones found in a mummy, through the first cautious surgeries of the nineteenth century, to the keyhole operation of the 1980s that turned gallbladder removal into one of the most common operations on Earth. Throughout, ancient finding of stones is kept carefully separate from the much later surgical milestones, dates are given as the historical record states them, and ideas that were guesses in their day are named as such.
Table of Contents
- Ancient Stones: The Egyptian Mummy and the Deep Past
- Medieval and Renaissance Autopsies
- The First Cautious Surgery: Petit and Bobbs
- Langenbuch and the First Cholecystectomy (1882)
- Cholesterol, Pigment, and the Chemistry of Stones
- The “Four F’s”: A Dated Teaching Mnemonic
- The Keyhole Revolution: Mühe and Mouret
- From Open Surgery to Modern Practice
- Research Papers and References
- Connections
- Featured Videos
Ancient Stones: The Egyptian Mummy and the Deep Past
Gallstones did not wait for modern diets to appear; they are as old as recorded humanity. The single most famous artifact in this story is a mummy from Deir el-Bahri at Thebes, identified in the surgical-history literature as a priestess of the twenty-first dynasty of ancient Egypt. When the body was examined, its preserved gallbladder was found to contain roughly thirty gallstones — an unmistakable case of cholelithiasis in a person who lived around three thousand years ago. In 1909 this mummified liver-and-gallbladder specimen was presented to the museum of the Royal College of Surgeons in London, where it became a celebrated piece of evidence that gallstone disease is genuinely ancient. (Readers should note a wrinkle in the dating: the surgical literature traditionally describes this priestess as living “around 1500 BCE,” but Egyptologists place the twenty-first dynasty considerably later, roughly 1069–945 BCE. The firm, repeatedly cited fact is the twenty-first-dynasty priestess and the 1909 presentation; the exact century is given here as the sources state it, with that caution.)
This was not a one-off curiosity. Gallstones have since been recovered from other ancient and historical human remains, including an eighteenth-century Sicilian mummy whose stones were studied by modern virtual-autopsy CT imaging, and from pre-Columbian mummies in South America. The lesson of these finds is consistent: stone formation in the gallbladder is a deep feature of human biology, not a purely modern affliction. It is, however, important to be precise about what these discoveries do and do not show. They tell us that stones existed in the bodies of ancient people; they do not tell us that those individuals were diagnosed, treated, or even troubled by them in life, since many gallstones cause no symptoms at all.
Written medicine took far longer to understand the organ than embalmers did to preserve it. Ancient Greek and Roman physicians wrote at length about bile — yellow bile and black bile were two of the four classical “humors” — and about jaundice and disorders they linked to the liver region, but a clear, specific account of stones lodged in the gallbladder belongs to a much later age. For most of antiquity, the small sac tucked under the liver, and the hard concretions it sometimes held, remained largely hidden from medical understanding even as the stones themselves were quietly being entombed.
Medieval and Renaissance Autopsies
The modern understanding of gallstones grew, slowly, out of the medieval and Renaissance revival of human dissection. A frequently cited early figure is the fourteenth-century Italian physician Gentile da Foligno, who is recorded as performing a human dissection (often dated to 1341) at a time when opening the body was still hedged about with taboo, and who is credited in the historical literature with an early postulated link between inflammation of the gallbladder and stones. Because the surviving accounts are second-hand and the medical vocabulary of the day was very different from ours, his contribution is best described as an early observation and hypothesis rather than a finished discovery — an honest reading of a fourteenth-century source.
Far clearer is the work of the Florentine physician Antonio Benivieni (who died in 1502), often called a father of pathological anatomy. Benivieni performed a series of autopsies — on the order of twenty — and recorded what he found, including gallstones. In at least one celebrated case he is said to have diagnosed gallstone disease in a living patient troubled by abdominal pain, a clinical impression then confirmed at autopsy — an early example of correlating symptoms in life with findings after death. His observations were published posthumously, and they mark the point where gallstones move from incidental curiosity to a recognized, describable disease of a specific organ.
The great anatomist Andreas Vesalius (1514–1564), whose richly illustrated De Humani Corporis Fabrica of 1543 reset the whole study of human anatomy, mapped the liver, the gallbladder, and the biliary ducts with new accuracy, giving later physicians a reliable picture of the structures in which stones form and the channels they can block. By the close of the Renaissance, then, three things were in place: dissection was respectable, the anatomy of the biliary tract was charted, and gallstones were a documented finding. What was still entirely missing was any safe way to do something about them in a living person.
The First Cautious Surgery: Petit and Bobbs
Surgery on the gallbladder lagged centuries behind the anatomy, for the obvious reason that opening the abdomen before anaesthesia and antisepsis was usually fatal. An important eighteenth-century step came from the French surgeon Jean-Louis Petit, who around 1743 described biliary colic and proposed that a gallbladder which had become stuck (adherent) to the abdominal wall might, in selected cases, be punctured to let stones and infected bile drain out. This was a cautious, staged idea suited to a pre-anaesthetic world, and it framed the gallbladder as something a surgeon might one day reach deliberately rather than only by accident.
The decisive early operation came in the United States. On 15 July 1867, in Indianapolis, Indiana, the surgeon John Stough Bobbs operated on a woman with a large abdominal swelling that proved to be a distended, stone-filled gallbladder (a hydrops). Expecting an ovarian cyst, Bobbs instead found the swollen gallbladder, opened it, removed the stones, and carefully sutured the organ closed — an operation we now call a cholecystotomy (or cholecystostomy: opening or draining the gallbladder). Crucially, Bobbs did not remove the gallbladder; he emptied it and left it in place. His patient survived and reportedly lived for many years, and the case earned Bobbs lasting recognition as a pioneer of biliary surgery. The distinction matters: Bobbs opened the gallbladder; he did not take it out.
This difference — opening and draining the organ versus removing it entirely — is the central conceptual divide in the history of gallbladder surgery. Bobbs and the surgeons who followed him in the 1870s, including the great Swiss surgeon Theodor Kocher who championed drainage of the gallbladder, treated the organ as something to be relieved and preserved. The bolder idea that the diseased, stone-making gallbladder should be removed altogether — root and branch — belonged to one man and one operation in Berlin.
Langenbuch and the First Cholecystectomy (1882)
The landmark of all gallbladder surgery is the work of the German surgeon Carl August Langenbuch (1846–1901). At the Lazarus Hospital in Berlin, on 15 July 1882 — by a striking coincidence, exactly fifteen years to the day after Bobbs’ cholecystotomy — Langenbuch performed the first planned cholecystectomy: the complete surgical removal of the gallbladder. His patient was a man who had suffered for years from gallstones; the operation succeeded, and the patient was discharged some weeks later. Langenbuch published the case the same year under the title “Ein Fall von Exstirpation der Gallenblase wegen chronischer Cholelithiasis” (“A case of extirpation of the gallbladder for chronic cholelithiasis”) in the Berliner Klinische Wochenschrift.
What makes Langenbuch a true pioneer is that the operation was not a lucky accident but the product of reasoning. He had argued from study of the organ’s function and from cadaver dissection that the gallbladder makes stones, that a person can live perfectly well without it, and that removing the stone-forming organ — rather than merely emptying it — was the rational cure. His famous principle, often paraphrased, was that the gallbladder should be removed not because it contains stones but because it forms them. That logic, validated by more than a century of practice, remains the foundation of gallstone surgery today: when symptomatic gallstones warrant an operation, the standard treatment is removal of the whole gallbladder.
For roughly a century after 1882, the open cholecystectomy Langenbuch devised — performed through a sizeable incision under the right ribs — was the definitive treatment for troublesome gallstones. It was effective and, as antisepsis and anaesthesia matured, increasingly safe, but it was major surgery: a long incision, a hospital stay of a week or more, and weeks of recovery. That was the unquestioned standard until a quiet revolution began, once again in Germany, in the 1980s.
Cholesterol, Pigment, and the Chemistry of Stones
While surgeons learned how to remove gallstones, chemists and pathologists worked out what they are made of — knowledge that explains who gets them and why. Gallstones are not all the same. The great majority in Western populations are cholesterol stones, which form when bile holds more cholesterol than it can keep dissolved, so that the excess crystallizes; these stones are typically pale yellow to greenish. A smaller share are pigment stones, made largely of bilirubin (the dark breakdown product of old red blood cells) combined with calcium. Pigment stones come in two flavors: black pigment stones, linked to conditions that break down red cells rapidly (such as certain anemias) or to cirrhosis, and brown pigment stones, associated with infection and stasis in the bile ducts. Many stones are in fact mixed.
This chemistry, worked out over the nineteenth and twentieth centuries, transformed a hard pebble into a readable record of a person’s metabolism. The identification of cholesterol as the dominant constituent of most Western gallstones tied the disease directly to cholesterol handling, bile composition, and how completely and how often the gallbladder empties — the physiological factors that govern whether dissolved cholesterol stays in solution or falls out as crystals. It also opened a non-surgical avenue: bile-acid medicines such as ursodeoxycholic acid can, in carefully chosen cases, slowly dissolve small cholesterol stones, although surgery remains the definitive treatment for stones that cause symptoms.
Understanding stone composition also clarified the targets of prevention and risk. Because cholesterol stones dominate, the conditions that raise biliary cholesterol or slow gallbladder emptying — and the populations in which they cluster — became the focus of risk research, which is where the much older bedside shorthand of the “four F’s” enters the story.
The “Four F’s”: A Dated Teaching Mnemonic
Generations of medical students have learned a memory aid for the classic gallstone patient: “fat, female, forty, and fertile” — the “four F’s,” sometimes stretched to five with the addition of “fair.” The mnemonic captures real and repeatedly observed associations: cholesterol gallstones are genuinely more common with higher body weight and obesity, in women (partly because of the effects of estrogen on bile), with increasing age, and in those who have been pregnant, since pregnancy alters bile composition and gallbladder emptying. As a quick reminder of well-established risk factors, it has a kernel of truth.
It must, however, be presented for exactly what it is: an old, deliberately crude teaching shorthand, and a potentially misleading one. Modern clinicians caution that leaning on the “four F’s” can breed bias — it can nudge a doctor toward the diagnosis in the stereotypical patient and, more dangerously, away from it in someone who does not fit the picture. Gallstones are common in men, in thin people, in the young, and in those who have never been pregnant. They are also notably frequent in particular populations not captured by the rhyme at all, such as several Native American and Hispanic groups, in whom genetics strongly raise the risk. The mnemonic is offered here as a historical artifact of medical teaching, useful for recalling a few risk factors, but never as a diagnostic rule and never as a reason to dismiss a person whose symptoms point to gallstones.
The Keyhole Revolution: Mühe and Mouret
The most dramatic change in gallbladder surgery since Langenbuch came in the 1980s, when the operation was reinvented as a keyhole (minimally invasive) procedure. The pioneer was the German surgeon Erich Mühe, who on 12 September 1985 performed what is now recognized as the world’s first laparoscopic cholecystectomy — removing a gallbladder through tiny incisions, guided by a viewing instrument, rather than through a long open cut. Inspired by the gynaecological laparoscopy of Kurt Semm, Mühe had designed his own instrument, which he called the “Galloscope,” and went on to perform many such operations. His pioneering role is well documented, but it was not initially honored: when he presented his results, much of the German surgical establishment dismissed the technique, and recognition came only years later — he was formally acknowledged for the first laparoscopic cholecystectomy in 1999.
The technique that swept the world, however, is most associated with the French surgeon Philippe Mouret, who in 1987 (his landmark case is dated to 17 March 1987) in Lyon performed a video-assisted laparoscopic cholecystectomy. Mouret’s work, soon taken up and refined by surgeons including François Dubois, Jacques Perissat, and others in France, the United States, and beyond, ignited an extraordinarily rapid global adoption. Within just a few years around 1990, laparoscopic cholecystectomy went from a fringe novelty to the new standard of care — one of the fastest transformations of a major operation in the history of surgery.
The reason for that speed was that the benefits to patients were immediate and obvious. Instead of a long incision, a week in hospital, and weeks of convalescence, the keyhole operation meant a few small puncture wounds, far less pain, often a same-day or overnight discharge, and a return to ordinary life in days. The historical fairness of giving Mühe his due while crediting Mouret with popularization is itself part of the story — a reminder that in medicine, being first and being recognized are not always the same thing.
From Open Surgery to Modern Practice
Today, laparoscopic cholecystectomy is among the most commonly performed operations in the world, with hundreds of thousands carried out each year in the United States alone. The open operation Langenbuch designed has not vanished — surgeons convert to an open approach when anatomy is unclear, when inflammation is severe, or when safety demands a direct view — but for the great majority of people with symptomatic gallstones, the keyhole procedure pioneered by Mühe and popularized by Mouret is the default. The whole long arc, from a priestess’s stones in a museum case to a forty-minute day-surgery procedure, is visible in a single modern operating room.
The diagnostic side of the story advanced just as far. Where Benivieni could only confirm a gallstone at autopsy, the twentieth century brought tools that find stones safely in living patients: the oral cholecystogram X-ray of the mid-century, and then the technology that changed everything, abdominal ultrasound, which from the 1970s onward made it possible to see gallstones quickly, cheaply, and without radiation. Ultrasound remains the first-line test for gallstones today, supplemented by CT, by MRCP (a magnetic-resonance picture of the bile ducts), and by ERCP, an endoscopic technique that can both image and clear stones lodged in the bile duct.
What endures from this long history are two simple, hard-won truths. First, that the rational treatment for a gallbladder that repeatedly makes painful stones is to remove the organ — Langenbuch’s 1882 insight, unchanged in principle after more than a century. Second, that the way to remove it should be as gentle on the patient as possible — the gift of Mühe and Mouret in the 1980s. The detailed modern picture of symptoms, diagnosis, complications such as cholecystitis and pancreatitis, and present-day treatment is covered on the main Gallbladder Disease page; this history exists to show how that hard-won knowledge was assembled, honestly and in order, over three thousand years.
Research Papers and References
The references below combine peer-reviewed historical and clinical reviews of gallstone disease and gallbladder surgery with curated PubMed topic-search links into the history and paleopathology literature. Where a specific paper is cited with a DOI or PMID, that identifier is given; broader historical claims (the twenty-first-dynasty mummy, the 1909 Royal College of Surgeons presentation, the early dissections of Gentile da Foligno and Benivieni) are supported through the named review literature and PubMed topic searches rather than asserted from a single primary source. Each external link opens in a new tab.
- Hardy KJ. Carl Langenbuch and the Lazarus Hospital: events and circumstances surrounding the first cholecystectomy. Australian and New Zealand Journal of Surgery. 1993;63(1):56-64. — PubMed PMID: 8466463
- Traverso LW. Carl Langenbuch and the first cholecystectomy. The American Journal of Surgery. 1976;132(1):81-82. — doi:10.1016/0002-9610(76)90295-6
- Reynolds W Jr. The first laparoscopic cholecystectomy. JSLS: Journal of the Society of Laparoendoscopic Surgeons. 2001;5(1):89-94. — Search PubMed
- Litynski GS. Erich Mühe and the rejection of laparoscopic cholecystectomy (1985): a surgeon ahead of his time. JSLS. 1998;2(4):341-346. — PubMed PMID: 10036125
- Blum CA, Adams DB. Who did the first laparoscopic cholecystectomy? Journal of Minimal Access Surgery. 2011;7(3):165-168. — Search PubMed
- Tanaja J, Lopez RA, Meer JM. Cholelithiasis. StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing. — NCBI Bookshelf: Cholelithiasis (StatPearls)
- History of gallstones and gallbladder surgery PubMed: history of gallstone surgery (Langenbuch, Bobbs)
- Gallstones in ancient Egyptian mummies and paleopathology PubMed: gallstones, mummies, and paleopathology
- Virtual-autopsy CT study of gallstones in a historical mummy PubMed: gallstones in a mummy (virtual autopsy / CT)
- Cholesterol versus pigment gallstones — composition and pathogenesis PubMed: cholesterol and pigment gallstone pathogenesis
- Risk factors for gallstone disease (the “four F’s” revisited) PubMed: gallstone risk-factor epidemiology
- History of laparoscopic surgery — Mühe, Mouret, and the keyhole revolution PubMed: history of laparoscopic cholecystectomy
- Andreas Vesalius and the anatomy of the biliary tract (history of anatomy) PubMed: Vesalius and the history of anatomy
- Ursodeoxycholic acid and non-surgical dissolution of cholesterol gallstones PubMed: bile-acid dissolution of cholesterol gallstones
External Authoritative Resources
Connections
- Gastroenterology
- Gallbladder Disease (main page)
- Gallstones — the stones at the centre of this history: how they form, and how they are found and treated today.
- All Conditions
- Pancreatitis — gallstones are a leading cause of acute pancreatitis
- Liver Disease — the liver makes the bile in which stones form
- Cirrhosis — associated with pigment gallstones
- Non-Alcoholic Fatty Liver Disease — shares metabolic risk factors with gallstones
- Hepatitis — another major disease of the liver and biliary system