Pemphigoid Gestationis
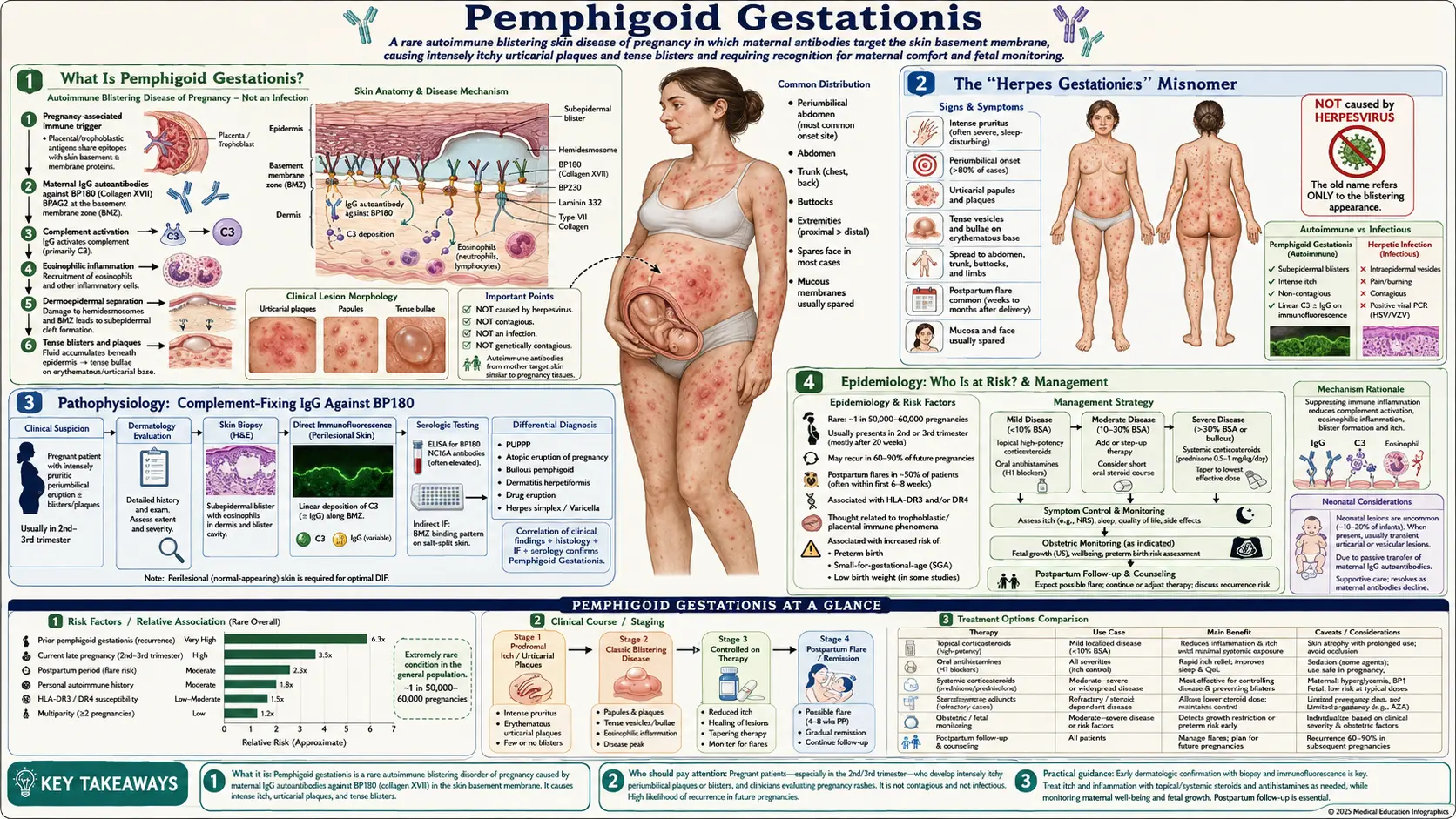
Pemphigoid gestationis (PG) is a rare, intensely pruritic autoimmune blistering disorder that occurs exclusively during pregnancy or in the immediate postpartum period. Despite its former name — herpes gestationis — the condition has no viral cause. It arises when maternal IgG antibodies attack a structural protein at the skin's basement membrane zone, triggering complement activation and a cascade of tissue destruction that produces the hallmark tense blisters. Understanding PG matters not only for the mother's comfort but because maternal antibodies cross the placenta and can briefly affect the newborn as well.
Table of Contents
- What Is Pemphigoid Gestationis?
- The "Herpes Gestationis" Misnomer
- Pathophysiology: Complement-Fixing IgG Against BP180
- Epidemiology: Who Is at Risk?
- Clinical Features and Periumbilical Origin
- Fetal and Neonatal Implications
- Diagnosis: C3 Linear Deposits and the HG Factor
- Treatment During and After Pregnancy
- Recurrence and Long-Term Outlook
- Key Research Papers
- Related PubMed Searches
- Featured Videos
What Is Pemphigoid Gestationis?
Pemphigoid gestationis is a pregnancy-specific autoimmune bullous (blistering) dermatosis classified within the pemphigoid family — the same family that includes bullous pemphigoid in older adults. The word gestationis simply means "of pregnancy," and the disease targets the same protein — collagen XVII, also called BP180 — attacked in bullous pemphigoid. What distinguishes PG is the unique immunological context of pregnancy: the placenta expresses BP180, offering a potential site of initial antigen presentation that sensitizes the maternal immune system.
The disease is remarkably rare. Estimates range from 1 case per 1,700 to 1 per 50,000 pregnancies, a wide range that reflects diagnostic heterogeneity across different centers and time periods. The cardinal symptom is intense, often intolerable pruritus that precedes the appearance of visible skin lesions. Early lesions look urticarial — red, swollen, hive-like — and are easily mistaken for the more common pruritic urticarial papules and plaques of pregnancy (PUPPP). The key distinguishing feature emerges later: PG progresses to form tense vesicles and bullae (blisters), while PUPPP does not blister.
The condition typically begins around the second or third trimester, with a mean onset near 21 weeks of gestation, though it can start at any point in pregnancy or even immediately after delivery. A characteristic paradoxical feature is postpartum flare: rather than improving after delivery of the placenta, many women experience their worst disease in the days immediately following birth before the condition gradually resolves over weeks to months.
The "Herpes Gestationis" Misnomer
For much of the twentieth century, pemphigoid gestationis was called herpes gestationis. This name created enormous confusion among patients and healthcare providers alike. The word "herpes" in this context was used in its oldest, purely descriptive sense — from the Greek word meaning "to creep," describing the way blisters seem to spread across the skin. It carried no implication of herpes simplex or herpes zoster viral infection.
However, as virology advanced and herpes simplex became associated primarily with sexually transmitted infections, the name "herpes gestationis" began to cause serious psychological distress. Pregnant women were sometimes incorrectly told, or feared, that they had contracted a viral sexually transmitted infection. The misunderstanding also led some clinicians to search needlessly for viral etiology and delay appropriate immunosuppressive treatment.
In 1983, the International Study Group on Pemphigoid Gestationis formally recommended retiring the name "herpes gestationis" in favor of "pemphigoid gestationis," reflecting its true nature as an autoimmune blistering disease in the pemphigoid family. This renaming emphasizes two key facts: the blistering mechanism (subepidermal, complement-mediated) is identical in mechanism to bullous pemphigoid, and the condition is entirely unrelated to any herpesvirus. Despite this formal change, the older name still appears in older literature and occasionally in clinical settings, which is why recognizing the equivalence matters.
Pathophysiology: Complement-Fixing IgG Against BP180
The central immunological event in pemphigoid gestationis is production of IgG1 autoantibodies directed against collagen XVII, also known as BP180 or BPAG2. This transmembrane protein spans the hemidesmosomes of basal keratinocytes and extends into the lamina lucida of the epidermal basement membrane zone (BMZ). It plays a structural role in anchoring the epidermis to the dermis. When antibodies bind BP180 — particularly targeting the NC16A domain — they trigger a sequence of events that dismantles this adhesion.
The critical antibody subclass is IgG1, which is a complement-fixing subclass. This is not a trivial detail: the ability to activate complement is what drives tissue damage. IgG1 autoantibodies binding to BP180 at the BMZ fix complement, activating the classical complement cascade and depositing C3 along the basement membrane zone. C3 deposition is present in virtually 100% of PG cases and is actually more reliably detected on direct immunofluorescence (DIF) than IgG itself. This makes C3 the more sensitive diagnostic marker.
The downstream effects of complement activation include mast cell degranulation, neutrophil and eosinophil recruitment, and release of proteolytic enzymes that cleave the lamina lucida. The result is separation of the epidermis from the dermis — a subepidermal split — producing the characteristic tense blister filled with clear fluid. Because the blister forms below the entire epidermis rather than within it, the roof remains intact and the blister appears tense rather than flaccid.
The placental connection is essential to understanding why this disease occurs in pregnancy at all. The amniotic epithelium and placental trophoblast express BP180/collagen XVII. This placental expression of the target antigen may provide the initial site of maternal immune sensitization — essentially, the placenta presents BP180 to the maternal immune system in the inflammatory context of early placentation, triggering production of anti-BP180 IgG1. The maternal antibodies then circulate to the skin and mount the destructive response there.
The historical term herpes gestationis factor (HG factor) refers to the complement-fixing IgG found in maternal serum — detectable by incubating patient serum with normal human skin sections in the presence of complement and observing C3 deposition at the BMZ. This factor represents the same anti-BP180 IgG1 autoantibody described above.
Epidemiology: Who Is at Risk?
Pemphigoid gestationis is rare by any measure. Incidence figures vary widely — from 1 in 1,700 to 1 in 50,000 pregnancies — reflecting genuine geographic and ethnic variability as well as differences in diagnostic rigor across studies. A reasonable working estimate for clinical purposes is approximately 1 in 10,000 to 1 in 50,000 pregnancies in Western populations.
Certain clinical patterns predict higher risk. Primigravidas (first-time pregnancies) are frequently affected. Intriguingly, women who become pregnant by a new partner appear at elevated risk compared to women in stable long-term relationships having a subsequent pregnancy. This has been interpreted through the lens of paternal antigen exposure: each new partner introduces new paternal HLA antigens into the trophoblast, potentially triggering a novel immune response against placental proteins.
Timing of onset clusters in the second and third trimesters, with a mean onset around 21 weeks. However, PG can begin in the first trimester, at delivery, or even in the immediate postpartum period. Two unusual associations deserve mention: PG has been documented in association with hydatidiform mole and choriocarcinoma — gestational trophoblastic diseases in which abnormal placental tissue proliferates without a viable fetus. This confirms that the antigenic stimulus arises from placental tissue, not from the fetus itself.
HLA typing in PG patients reveals a striking association with HLA-DR3 and HLA-DR4. Women carrying both alleles (DR3/DR4) are particularly predisposed — the same allelic combination linked to type 1 diabetes and other autoimmune conditions. This HLA association underscores the autoimmune nature of PG and explains why affected women have higher lifetime rates of other autoimmune diseases, particularly autoimmune thyroid disease.
After a first affected pregnancy, recurrence in subsequent pregnancies is almost universal. Recurrences tend to begin earlier in gestation and may be more severe than the index episode. Between pregnancies, some women experience transient disease reactivation with menses or after taking estrogen-containing oral contraceptives — a phenomenon that highlights the role of sex hormone fluctuation in modulating the autoimmune response.
Clinical Features and Periumbilical Origin
The clinical presentation of pemphigoid gestationis evolves in two recognizable phases. The early phase can be deceptively similar to other pregnancy dermatoses; the later blistering phase is more distinctive.
Prodromal Urticarial Phase
The first lesions are intensely pruritic urticarial papules and plaques — red, raised, hive-like eruptions that may coalesce into large, polycyclic patches. At this stage, PG is clinically indistinguishable from PUPPP (pruritic urticarial papules and plaques of pregnancy), which is far more common. The pruritus in PG is typically severe, often described by patients as among the most intense itching they have experienced, and frequently disrupts sleep.
The hallmark of this early stage is the anatomical starting point: the eruption classically begins in and around the umbilicus. The periumbilical distribution is characteristic enough that it is taught as a diagnostic clue — PG starts at the navel and spreads outward to the trunk, thighs, arms, and eventually the palms and soles. PUPPP, by contrast, typically begins in abdominal striae and characteristically spares the periumbilical skin.
Blistering Phase
Over days to weeks, the urticarial lesions evolve into tense vesicles and bullae. The word "tense" is key — because the blister forms below the full thickness of the epidermis (subepidermal), the roof is tough and intact, and the blister does not easily rupture when pressed. This contrasts with intraepidermal blisters (as in pemphigus), which are flaccid and fragile.
The distribution in the blistering phase encompasses the trunk, extremities, palms, and soles. Mucous membranes are typically spared in PG, which distinguishes it from mucous membrane pemphigoid (formerly called cicatricial pemphigoid) and from some other bullous diseases. The face is usually not prominently affected.
Postpartum Flare
One of the most clinically important features of PG is the paradoxical postpartum flare. Rather than improving immediately after delivery — as might be expected when the antigenic placental stimulus is removed — many women experience their most severe disease in the days and weeks after birth. This worsening may reflect a rebound immunological response as immunosuppression that existed during pregnancy lifts. The flare gradually resolves over weeks to months in most cases. Breastfeeding does not appear to significantly affect the course.
Estrogen Sensitivity
Outside of pregnancy, women with a history of PG may experience disease reactivation with menses or after starting estrogen-containing oral contraceptives. This sensitivity to estrogen is a practical concern for contraception counseling after delivery — progesterone-only methods are generally preferred.
Fetal and Neonatal Implications
Because pemphigoid gestationis involves IgG1 antibodies — a subclass that efficiently crosses the placenta via neonatal Fc receptors — the disease has implications beyond the mother's skin.
Neonatal Pemphigoid Gestationis
Approximately 2 to 5 percent of neonates born to mothers with PG develop transient blistering skin lesions at birth or in the first days of life. This neonatal PG results directly from transplacental passage of maternal anti-BP180 IgG1, which temporarily attacks the newborn's own skin basement membrane. Reassuringly, neonatal PG is self-limiting: as maternal antibody is gradually catabolized, blistering resolves spontaneously over weeks without lasting skin damage. No active treatment beyond supportive wound care is generally needed. Parents should be counseled before delivery about the possibility of neonatal blistering so they are not alarmed at birth.
The severity of neonatal PG does not correlate perfectly with maternal disease severity, and neonates can be affected even when maternal disease is relatively mild or predominantly urticarial.
Small for Gestational Age and Prematurity
Studies have documented a moderate association between PG and small for gestational age (SGA) infants. Complement-mediated damage at the placental basement membrane — the same mechanism that causes skin blistering — may impair uteroplacental blood flow, restricting fetal growth. Prematurity has also been reported, though it is unclear how much reflects spontaneous preterm labor versus iatrogenic delivery for disease severity.
Overall, neonatal prognosis is excellent. The transient blistering is alarming to witness but resolves completely. Long-term follow-up studies do not show excess neonatal morbidity or developmental problems in children born to PG-affected mothers.
Implications for Obstetric Management
Women with PG should receive enhanced fetal monitoring including growth scans to assess for SGA. Neonatology teams benefit from advance notification when a PG mother is delivering so that neonatal skin examination is thorough and appropriate follow-up is arranged. Breastfeeding is generally permitted; the clinical relevance of maternal antibodies in breast milk is considered low.
Diagnosis: C3 Linear Deposits and the HG Factor
Accurate diagnosis of pemphigoid gestationis requires integrating clinical features with immunopathological testing. The diagnosis should be suspected in any pregnant woman with intensely pruritic urticarial lesions, particularly with periumbilical onset or progression to tense blisters.
Skin Biopsy: Histopathology
A punch biopsy from an early lesion (urticarial, not an established blister) shows eosinophilic spongiosis and a dermal infiltrate rich in eosinophils. An established blister biopsy demonstrates subepidermal cleavage — the split occurs below the entire epidermis at the level of the lamina lucida — with eosinophil-rich inflammation. These histological findings are consistent with but not specific for PG; they overlap with bullous pemphigoid and other subepidermal bullous diseases.
Direct Immunofluorescence (DIF): C3 Is Key
DIF on perilesional skin is the diagnostic cornerstone. The finding is linear C3 deposition along the basement membrane zone, present in virtually 100% of PG cases. Linear IgG deposition is found in approximately 60 to 90% of cases, making C3 more sensitive than IgG for PG diagnosis by DIF.
This is a clinically important distinction: if DIF shows only C3 without detectable IgG, the diagnosis of PG remains valid when the clinical context (pregnant woman, periumbilical onset, tense blisters) is compatible. A result showing only C3 is not a "partial" or "equivocal" result — C3 alone is sufficient. Compare this to bullous pemphigoid, which shows both IgG and C3 linear deposits, though the distinction between BP and PG is ultimately made by clinical context (pregnant vs. non-pregnant, typical age, etc.) rather than by immunofluorescence pattern alone.
Indirect Immunofluorescence: The HG Factor
Patient serum contains the so-called herpes gestationis (HG) factor — the complement-fixing IgG1 anti-BP180 antibody. Indirect immunofluorescence (IIF) using normal human skin substrate in the presence of exogenous complement demonstrates C3 deposition at the BMZ, confirming circulating complement-activating antibody. This test is positive in the majority of active cases but is less widely available than ELISA-based assays.
ELISA: Anti-BP180 IgG (NC16A Domain)
Commercial ELISA assays measuring anti-BP180 IgG, targeting the immunodominant NC16A domain, offer a practical serological confirmation. Sensitivity is approximately 80 to 90% in active PG. Anti-BP230 antibodies may be co-present. Antibody titers can roughly correlate with disease activity, making them useful for monitoring.
Distinguishing PG from PUPPP
The critical differential diagnosis in the urticarial phase is PUPPP. Key distinctions:
- Periumbilical onset: PG starts around the umbilicus; PUPPP typically starts in striae and classically spares periumbilical skin.
- Blistering: PG progresses to tense bullae; PUPPP does not blister.
- DIF: PG shows C3 (and often IgG) linear at BMZ; PUPPP has negative DIF.
- Recurrence: PG almost always recurs in subsequent pregnancies; PUPPP does not.
- Timing: PUPPP is predominantly third-trimester and most common in primigravidas, often resolving within days of delivery without postpartum flare.
Treatment During and After Pregnancy
Treatment is guided by disease severity, gestational age, and the safety profile of medications in pregnancy. The overall goals are controlling pruritus, preventing new blister formation, and protecting skin integrity — while minimizing fetal exposure to immunosuppressants.
Mild Disease: Urticarial Phase Without Bullae
Potent topical corticosteroids (such as clobetasol propionate or betamethasone dipropionate) applied to active urticarial lesions are the first-line treatment for mild PG. Localized topical corticosteroids have minimal systemic absorption and minimal fetal risk when used on limited skin areas.
Oral antihistamines provide symptomatic pruritus relief but do not modify the underlying immune response. Cetirizine and loratadine are generally preferred in the second and third trimesters. Chlorphenamine (chlorpheniramine) may be used in the first trimester if needed. Sedating antihistamines near delivery are generally avoided because of neonatal sedation risk.
Moderate to Severe Disease: Bullae or Extensive Involvement
Systemic corticosteroids are the mainstay of moderate to severe PG. Prednisolone is preferred over prednisone during pregnancy because prednisolone is the active metabolite and crosses the placenta less efficiently (the placenta converts prednisolone back to prednisone, reducing fetal exposure). A starting dose of 0.5 mg/kg/day prednisolone is commonly used, with tapering as the disease responds. The goal is the minimum dose that controls new blister formation.
Long-term corticosteroid use in pregnancy carries risks including gestational diabetes, hypertension, infection, adrenal suppression, and (for the fetus) SGA — these must be monitored and weighed against disease severity. Doses below 10 mg/day prednisolone are considered relatively low risk.
Refractory Disease and Postpartum Options
For disease that does not respond to systemic corticosteroids, or for managing severe postpartum disease when teratogenicity is no longer a concern, several options exist:
- Intravenous immunoglobulin (IVIg): Case reports and small series support IVIg in refractory PG, both during pregnancy and postpartum. The mechanism likely involves Fc receptor saturation and accelerated catabolism of pathogenic IgG.
- Rituximab: The anti-CD20 monoclonal antibody that depletes B cells has been used postpartum in refractory cases. It is not generally used during pregnancy because of potential effects on fetal B-cell development.
- Dapsone: Effective in many bullous diseases; however, dapsone carries risk of hemolytic anemia in the neonate (especially in G6PD deficiency) and is generally avoided during pregnancy and when breastfeeding. It may be considered postpartum in non-breastfeeding women.
- Plasmapheresis: Mechanical removal of circulating antibodies; used in severe cases, typically postpartum or in life-threatening gestational disease.
Contraception After Delivery
Because estrogen-containing oral contraceptives can trigger PG reactivation or postpartum flare, progesterone-only methods (progesterone-only pill, intrauterine device, depot injection) are preferred for contraception in women with PG history. This counseling should be offered before hospital discharge after delivery.
Wound Care
When blisters are present, intact tense bullae should generally be left intact if possible to reduce infection risk. Ruptured blisters should be covered with non-adherent dressings. Skin superinfection with Staphylococcus aureus is the most common complication and should be treated promptly with appropriate antibiotics.
Recurrence and Long-Term Outlook
Pemphigoid gestationis almost invariably recurs in subsequent pregnancies. Recurrences tend to begin earlier in gestation than the initial episode and may be more severe. This "priming" effect is attributed to pre-existing maternal B-cell memory for anti-BP180 IgG: when a new pregnancy restimulates placental BP180 antigen presentation, the secondary antibody response is faster and stronger. Women planning subsequent pregnancies should be counseled about near-certain recurrence and have a dermatologist involved in prenatal care from early in subsequent gestations.
Between pregnancies, most women are entirely asymptomatic. However, a minority experience ongoing pruritus or periodic urticarial flares — particularly around menses or after initiating estrogen-containing contraceptives. This estrogen sensitivity reflects the hormonal modulation of the underlying autoimmune state. Progesterone-only contraception mitigates this risk.
Autoimmune Thyroid Disease
Women with a history of PG carry a measurably elevated risk of autoimmune thyroid disease — particularly Graves' disease and Hashimoto's thyroiditis. This association likely reflects shared HLA predisposition (HLA-DR3/DR4) to multiple autoimmune conditions. Annual thyroid function testing (TSH) is a reasonable precaution in the years following a PG pregnancy.
Long-Term Skin Prognosis
Once PG resolves — which it does in essentially all cases, typically over weeks to months postpartum — there are no lasting skin sequelae. PG does not cause scarring under most circumstances, though resolving blisters may leave temporary post-inflammatory hyperpigmentation that fades over months. Unlike some other autoimmune blistering diseases, PG does not progress to a chronic non-pregnancy-related bullous disease in the vast majority of patients.
Fetal and Neonatal Long-Term Outlook
The neonatal blistering that occurs in 2 to 5 percent of infants resolves completely without long-term sequelae. Follow-up studies have not identified developmental, immunological, or skin abnormalities in children born to PG-affected mothers. Once maternal IgG clears from the neonatal circulation — typically over the first weeks to months of life — the neonate's own immune system does not perpetuate the anti-BP180 response.
Key Research Papers
- Shornick JK. "Herpes gestationis." J Am Acad Dermatol. 1987;17(4):539–556. — Search PubMed
- Ambros-Rudolph CM, Müllegger RR, Vaughan-Jones SA, et al. "The specific dermatoses of pregnancy revisited and reclassified: results of a retrospective two-center study on 505 pregnant patients." J Am Acad Dermatol. 2006;54(3):395–404. — Search PubMed
- Jenkins RE, Hern S, Black MM. "Clinical features and management of 87 patients with pemphigoid gestationis." Clin Exp Dermatol. 1999;24(4):255–259. — Search PubMed
- Semkova K, Black M. "Pemphigoid gestationis: current insights into pathogenesis and treatment." Eur J Obstet Gynecol Reprod Biol. 2009;145(2):138–144. — Search PubMed
- Sitaru C, Powell J, Messer G, et al. "Immunoblotting and enzyme-linked immunosorbent assay for the diagnosis of pemphigoid gestationis." Obstet Gynecol. 2004;103(4):757–763. — Search PubMed
- Intong LR, Murrell DF. "Pemphigoid gestationis: pathogenesis and clinical features." Dermatol Clin. 2011;29(3):447–452. PMID: 21605807
- Mokni M, Fourati M, Karoui N, et al. "IgG anti-BP180 autoantibodies are characteristic of pemphigoid gestationis." Ann Dermatol Venereol. 2010;137(2):97–101. — Search PubMed
- Shornick JK, Bangert JL, Freeman RG, et al. "Herpes gestationis: clinical and histologic features of twenty-eight cases." J Am Acad Dermatol. 1983;8(2):214–224. — Search PubMed
- Chimanovitch I, Schmidt E, Messer G, et al. "IgG1 and IgG3 are the predominant IgG subclasses of BP180 reactive antibodies in pemphigoid gestationis." J Invest Dermatol. 1999;113(1):140–142. PMID: 10417632
- Ambros-Rudolph CM. "Dermatoses of pregnancy — clues to diagnosis, fetal risk and therapy." Ann Dermatol. 2011;23(3):265–275. — Search PubMed
- Hallaji Z, Mortazavi H, Ashtari S, et al. "Pemphigoid gestationis: a clinical and immunological study of 35 cases." Int J Womens Dermatol. 2017;3(2):86–90. — Search PubMed
- Krishnan RS, Lawley TJ. "Pemphigoid gestationis." Semin Dermatol. 1992;11(1):12–16. — Search PubMed
Related PubMed Searches
- Pemphigoid gestationis — PubMed search
- Herpes gestationis autoimmune — PubMed search
- BP180 collagen XVII pregnancy antibody — PubMed search
- Bullous dermatosis pregnancy diagnosis — PubMed search
- Neonatal pemphigoid gestationis transplacental — PubMed search
Connections
- Dermatology
- Dermatitis Herpetiformis
- Linear IgA Bullous Dermatosis
- Epidermolysis Bullosa
- Diseases — Main Index
- Gastroenterology — Disease Index