Abdominal Pain
Abdominal pain is one of the most common presenting complaints in emergency departments and primary care, accounting for more than 8 million emergency visits annually in the United States. It spans a spectrum from benign functional disorders to immediately life-threatening surgical emergencies. Accurate localization, pattern recognition, and systematic clinical assessment are essential to distinguish conditions that require urgent intervention from those that can be managed conservatively.
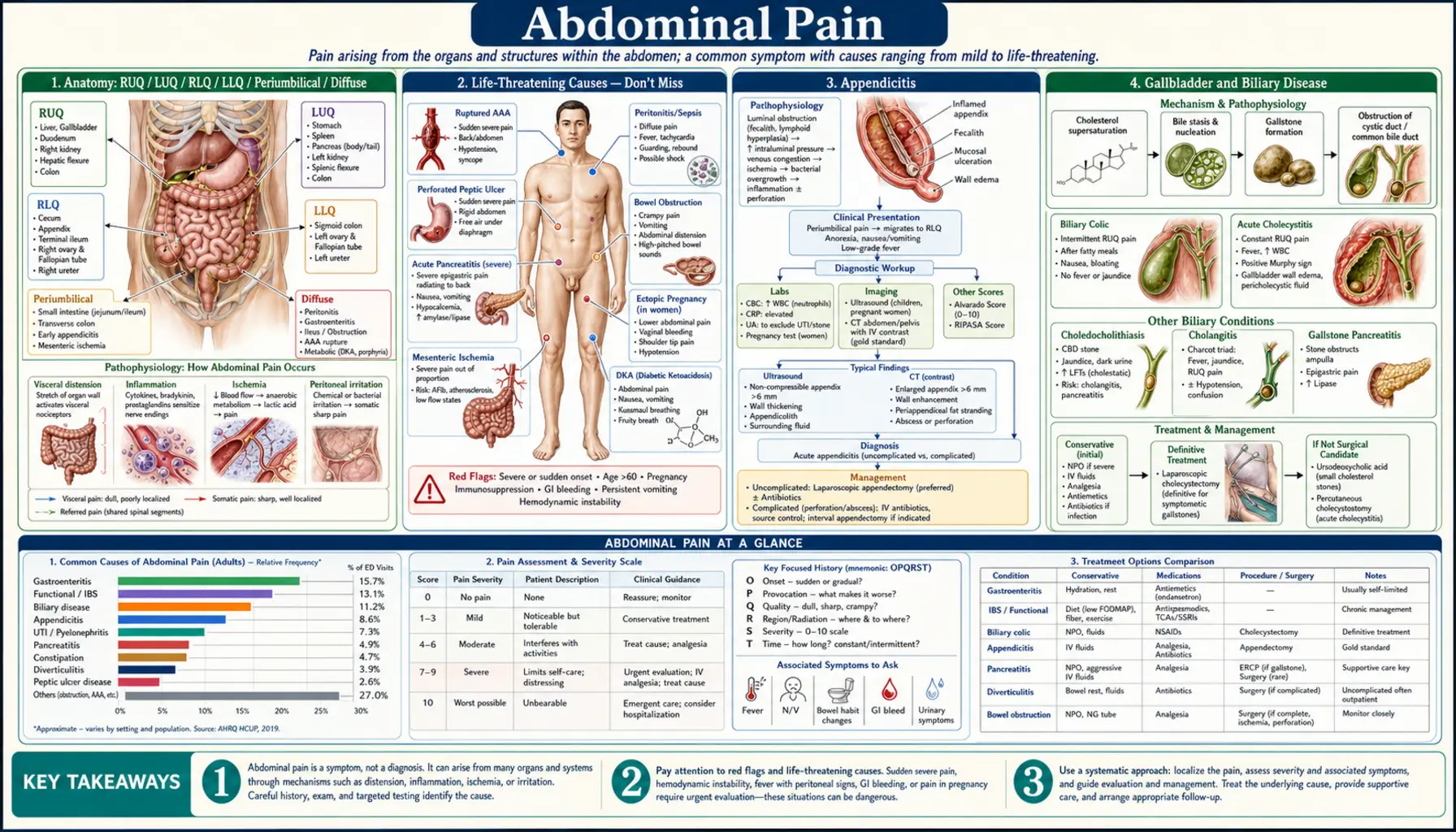
Anatomy: RUQ / LUQ / RLQ / LLQ / Periumbilical / Diffuse
Localizing abdominal pain to a quadrant or region is the first and most critical step in narrowing the differential diagnosis. Each quadrant contains specific anatomical structures whose pathology produces characteristic pain patterns. Understanding referred pain (diaphragmatic irritation → shoulder pain; pelvic pathology → inner thigh) further expands the diagnostic framework.
Right Upper Quadrant (RUQ)
- Biliary: Cholecystitis (Murphy's sign positive; gallbladder wall inflammation); choledocholithiasis (common bile duct stone; jaundice + elevated ALP/GGT); cholangitis (Charcot's triad: fever + jaundice + RUQ pain)
- Liver: Hepatitis (viral or toxic; diffuse hepatic enlargement; RUQ fullness + tenderness); hepatic abscess (fever + RUQ pain + elevation of right hemidiaphragm on imaging); hepatomegaly from any cause (heart failure; infiltrative disease)
- Pulmonary: Right lower lobe pneumonia causes referred RUQ pain via diaphragmatic irritation — always consider in patients with fever + RUQ pain + respiratory symptoms
- Cardiac: Right heart failure causes hepatic venous congestion → tender, enlarged liver + RUQ fullness; distinguishable by JVD, peripheral edema, and echocardiography
- Peptic: Peptic ulcer disease involving the first portion of the duodenum or the antrum of the stomach may produce RUQ/epigastric radiation
Left Upper Quadrant (LUQ)
- Spleen: Splenomegaly (EBV mononucleosis; hematologic malignancy; portal hypertension); splenic infarct (sickle cell; embolic disease; LUQ pain + fever); spontaneous splenic rupture (EBV; trauma; rarely warfarin) — can be life-threatening
- Gastric: Gastric ulcer (pain with eating; H. pylori; NSAIDs; risk of bleeding and perforation); gastric outlet obstruction (projectile vomiting; succussion splash)
- Pancreatic: The tail of the pancreas lies in the LUQ; acute pancreatitis pain can be epigastric radiating to the LUQ and through to the back
- Pulmonary: Left lower lobe pneumonia can cause referred LUQ pain via left hemidiaphragm irritation
Right Lower Quadrant (RLQ)
- Appendicitis: The most feared RLQ diagnosis; pain migrates from periumbilical to RLQ (McBurney's point: 1/3 of the way from the anterior superior iliac spine to the umbilicus); Rovsing's sign (LLQ pressure elicits RLQ pain); psoas sign (retrocecal appendix); obturator sign (pelvic appendix)
- Ovarian/Adnexal: Ovarian torsion (sudden severe unilateral pain + nausea; requires urgent surgical intervention); ruptured ovarian cyst (acute onset; may resolve spontaneously); ectopic pregnancy (always rule out in women of childbearing age)
- Inguinal hernia: Reducible vs. incarcerated vs. strangulated; strangulated hernia = surgical emergency (ischemic bowel)
- Crohn's disease: Terminal ileum is the most commonly affected segment; RLQ pain + diarrhea + weight loss; "string sign" on imaging
- Mesenteric lymphadenitis: Viral infection → enlarged mesenteric nodes; most common cause of RLQ pain in children after appendicitis; self-limiting; difficult to distinguish from appendicitis without imaging
Left Lower Quadrant (LLQ)
- Diverticulitis: Sigmoid colon diverticula (most common location); LLQ pain + fever + elevated WBC; high-fiber diet is protective; CT abdomen/pelvis is gold standard; managed with antibiotics for uncomplicated disease; complications: abscess, perforation, fistula, obstruction
- Ovarian (left-sided): Same spectrum as RLQ ovarian pathology; always obtain urine pregnancy test and pelvic ultrasound
- Constipation: Hard stool impaction in the sigmoid colon causes LLQ fullness and cramping; distinguishable by history and plain abdominal X-ray showing stool burden
Periumbilical
- Small bowel obstruction: Crampy periumbilical pain + distension + vomiting + obstipation; adhesions are the most common cause in adults; air-fluid levels on KUB
- Early appendicitis: Visceral pain originates at the periumbilical region via T10 dermatome before localizing to RLQ as the parietal peritoneum becomes involved
- Aortic: Abdominal aortic aneurysm (AAA); pulsatile midline mass; tearing or severe periumbilical pain is an emergency; elderly men with smoking history
- Umbilical hernia: Incarcerated or strangulated umbilical hernias require urgent surgical evaluation
Diffuse Abdominal Pain
- Peritonitis: Rebound tenderness + guarding + rigidity; involuntary guarding = parietal peritoneum involvement; causes include perforated viscus, ruptured appendix, ruptured ectopic pregnancy
- Gastroenteritis: Diffuse cramping + nausea/vomiting + diarrhea; usually viral (norovirus; rotavirus); foodborne bacterial (Salmonella; Campylobacter; E. coli O157:H7)
- Irritable Bowel Syndrome: Diffuse cramping without localization; associated with bowel habit changes; no structural cause; highly prevalent (10-15% worldwide)
- Mesenteric ischemia: Severe diffuse pain out of proportion to exam findings; older patients with atrial fibrillation or atherosclerosis; elevated lactate; surgical emergency
- Diabetic ketoacidosis: DKA causes diffuse abdominal pain in up to 50% of cases via gastric paresis and mesenteric vasoconstriction; always check glucose and pH in abdominal pain patients with diabetes
Life-Threatening Causes — Don't Miss
A subset of abdominal pain presentations represent immediate surgical or vascular emergencies where delay in diagnosis directly increases mortality. These diagnoses must be considered in every patient with acute abdominal pain and explicitly ruled in or out before discharge.
Ruptured Abdominal Aortic Aneurysm (AAA)
The classic triad is sudden severe abdominal or back pain + hypotension + pulsatile abdominal mass. Ruptured AAA carries an overall mortality of approximately 85%, and even with immediate surgical intervention, operative mortality approaches 50%. Risk factors include elderly male sex, smoking history, hypertension, and known aneurysm. Hemodynamically unstable patients should go directly to the operating room without CT delay. Stable patients may undergo CTA for anatomic planning. Bedside ultrasound can rapidly confirm AAA presence (sensitivity >95% for aneurysm diameter) but cannot reliably detect retroperitoneal rupture.
Mesenteric Ischemia
The hallmark is pain out of proportion to physical examination — the patient appears to be in agony but the abdomen may be soft and non-tender on palpation initially. Acute mesenteric ischemia most commonly results from embolic occlusion of the superior mesenteric artery (SMA), often in patients with atrial fibrillation. Chronic mesenteric ischemia (intestinal angina) presents as postprandial pain and weight loss from atherosclerotic disease. Laboratory findings include elevated lactate and leukocytosis. CT angiography is the diagnostic study of choice. Without prompt revascularization, bowel necrosis → peritonitis → multiorgan failure → death.
Bowel Obstruction with Strangulation
Simple mechanical obstruction presents with colicky pain, distension, vomiting, and obstipation. When strangulation occurs (vascular compromise of the bowel wall), the pain changes from colicky to constant, peritoneal signs develop, fever and leukocytosis appear, and the patient becomes hemodynamically unstable. Multiple air-fluid levels on plain X-ray and CT confirm obstruction. Strangulated bowel requires immediate surgical exploration — bowel necrosis progresses rapidly to perforation and sepsis.
Ectopic Pregnancy
Any woman of childbearing age presenting with abdominal pain and amenorrhea must be considered to have an ectopic pregnancy until proven otherwise. Serum beta-hCG combined with transvaginal ultrasound is the diagnostic standard. An adnexal mass without intrauterine pregnancy on ultrasound with a positive beta-hCG is ectopic until proven otherwise. Rupture causes hemoperitoneum, hemorrhagic shock, and death if not treated emergently. Unruptured ectopic pregnancy can be managed medically (methotrexate) or surgically (salpingostomy or salpingectomy).
Perforated Viscus
Perforation of the stomach or duodenum (from peptic ulcer disease), colon (from diverticulitis or malignancy), or appendix causes sudden onset severe diffuse abdominal pain. The abdomen becomes board-like rigid. Free air under the diaphragm on upright chest X-ray (Rigler's sign on supine films) confirms the diagnosis. CT is more sensitive than plain films. Emergency surgery is required. Delay results in fecal peritonitis, overwhelming sepsis, and death.
Appendicitis
Acute appendicitis is the most common surgical emergency in the United States, with a lifetime risk of approximately 7%. It occurs most frequently in the second and third decades of life but can affect any age group. Prompt diagnosis prevents the 25-30% perforation rate that dramatically increases morbidity, hospital length of stay, and mortality.
Pathophysiology
Luminal obstruction of the appendix — most commonly by a fecalith, lymphoid hyperplasia (in children and young adults), or foreign body — leads to bacterial overgrowth and mucus accumulation. Elevated intraluminal pressure impairs venous drainage, causing ischemia, transmural inflammation, and ultimately perforation if untreated. The appendix perforates into the peritoneal cavity (causing diffuse peritonitis) or becomes walled off by omentum (forming a periappendiceal abscess).
Clinical Presentation
- Periumbilical pain migrating to RLQ: Visceral pain (T10 dermatome) presents first as dull periumbilical discomfort, then localizes to RLQ (Kosher's sign) as the parietal peritoneum becomes inflamed
- Anorexia: Present in approximately 95% of cases; its absence should prompt reconsideration of the diagnosis
- Nausea and vomiting: Usually follow the onset of pain (pain before vomiting distinguishes appendicitis from gastroenteritis, where vomiting typically precedes or accompanies pain)
- Fever: Low-grade initially (37.5–38.5°C); high fever suggests perforation or abscess formation
Physical Examination Signs
- McBurney's point tenderness: Maximum tenderness at a point 1/3 of the way from the anterior superior iliac spine (ASIS) to the umbilicus
- Rovsing's sign: Palpation of the LLQ elicits pain in the RLQ; indicates peritoneal irritation in the RLQ
- Psoas sign: Extension of the right hip against resistance elicits RLQ pain; suggests retrocecal appendix with psoas muscle irritation
- Obturator sign: Internal rotation of the flexed right hip elicits RLQ/hypogastric pain; suggests pelvic appendix
Alvarado Score (MANTRELS)
A validated clinical scoring system to risk-stratify appendicitis:
- Migration of pain to RLQ (1 point)
- Anorexia (1 point)
- Nausea/vomiting (1 point)
- Tenderness in RLQ (2 points)
- Rebound tenderness (1 point)
- Elevated WBC >10,000 (2 points)
- Left shift (elevated neutrophil percentage) (1 point)
Score 7–10 = high risk (surgical consultation without mandatory CT); score 4–6 = intermediate risk (CT recommended); score 1–3 = low risk (observation, discharge with return precautions).
Imaging
- CT abdomen/pelvis with IV contrast: Gold standard; sensitivity 92–97%, specificity 94–97%; visualizes inflamed appendix (diameter >6 mm, periappendiceal fat stranding, fecalith, abscess, perforation)
- Ultrasound: First-line in children and pregnant women (avoids radiation); operator-dependent; non-visualization of appendix does not exclude appendicitis
- MRI: Preferred in pregnancy when ultrasound is non-diagnostic; high sensitivity without radiation exposure
Treatment: Surgery vs. Antibiotics
Laparoscopic appendectomy remains the gold standard treatment. However, the landmark APPAC trial (JAMA 2015) and subsequent CODA trial (NEJM 2020) demonstrated that antibiotic-first therapy is a viable option for selected patients with uncomplicated (non-perforated) appendicitis. In the APPAC trial, 73% of the antibiotic group avoided surgery at 30 days, though 29% experienced recurrence within one year. Patients and physicians can engage in shared decision-making regarding operative versus non-operative management for uncomplicated appendicitis. Complicated appendicitis (perforation, abscess, peritonitis) requires surgery.
Gallbladder and Biliary Disease
Biliary tract disease is one of the most common causes of acute abdominal pain requiring hospital admission, responsible for more than 200,000 cholecystectomies annually in the United States. Understanding the clinical spectrum from biliary colic to cholangitis is essential for appropriate triage and management.
Biliary Colic
Biliary colic results from episodic impaction of a gallstone at the neck of the gallbladder or cystic duct, triggered by cholecystokinin release after fatty meals. The pain is typically constant (not truly colicky despite the name), builds over 15–30 minutes, reaches a plateau, and resolves over 1–6 hours as the stone falls back into the gallbladder lumen. Radiation to the right shoulder or interscapular region occurs via phrenic nerve irritation. Nausea is common; fever and leukocytosis are absent. Ultrasound is the first-line imaging study, with 95% sensitivity for gallstones.
Acute Cholecystitis
Sustained impaction of a stone in the cystic duct leads to prolonged gallbladder distension, secondary bacterial infection, and transmural inflammation. Unlike biliary colic, cholecystitis causes persistent RUQ pain (>6 hours), fever, and leukocytosis. Murphy's sign is the clinical hallmark: deep inspiration during RUQ palpation causes pain and inspiratory arrest as the inflamed gallbladder descends into the examiner's fingers. Ultrasound findings include gallbladder wall thickening (>4 mm), pericholecystic fluid, and a sonographic Murphy's sign. Treatment is IV antibiotics followed by laparoscopic cholecystectomy (within 72 hours of admission in most cases).
Choledocholithiasis
Migration of a gallstone into the common bile duct (CBD) causes biliary obstruction with RUQ pain, jaundice, elevated serum bilirubin, alkaline phosphatase (ALP), and gamma-glutamyl transferase (GGT). Aminotransferases (AST/ALT) may be transiently elevated. ERCP (endoscopic retrograde cholangiopancreatography) is both diagnostic and therapeutic for CBD stone removal.
Acute Cholangitis
Bacterial infection of an obstructed biliary tree constitutes a medical and surgical emergency. Charcot's triad — fever/rigors + jaundice + RUQ pain — is present in approximately 70% of cases. Reynolds's pentad — Charcot's triad + septic shock + altered mental status — indicates severe cholangitis with high mortality and mandates urgent biliary decompression via ERCP or percutaneous transhepatic cholangiography (PTC). Blood cultures should be drawn before antibiotics; broad-spectrum coverage including gram-negative organisms and anaerobes is standard.
Peptic Ulcer Disease and GERD
Peptic ulcer disease (PUD) affects approximately 4.5 million Americans annually. Helicobacter pylori infection and NSAID use account for the majority of cases. Understanding the distinct pain patterns of gastric versus duodenal ulcers is a classic clinical differentiator.
Gastric Ulcer
Gastric ulcers cause epigastric or LUQ pain that characteristically worsens with eating (food stimulates acid secretion → pain; food avoidance → weight loss). H. pylori accounts for approximately 70% of gastric ulcers; NSAIDs (which suppress prostaglandin-mediated mucosal protection) account for much of the remainder. Risk factors include smoking, alcohol, and physiological stress (stress ulcers in ICU patients). Complications include:
- Bleeding: Hematemesis (bright red blood or "coffee grounds") + melena (tarry black stool) + iron-deficiency anemia; most common complication; urgent endoscopy for hemostasis
- Perforation: Sudden onset diffuse severe pain + board-like rigidity + free air under diaphragm on upright CXR; requires emergency surgery
- Gastric outlet obstruction: Chronic scarring from repeated ulcers at the pylorus → projectile vomiting + succussion splash + metabolic alkalosis (from vomiting of HCl)
Duodenal Ulcer
Duodenal ulcers produce pain 2–3 hours after eating (when the stomach is empty and acid contact with the duodenal mucosa is maximal) and classically awaken the patient from sleep (nocturnal pain). Pain is characteristically relieved by eating (food buffers acid). H. pylori is present in approximately 95% of duodenal ulcer patients. The pain is typically epigastric and burning in character.
Diagnosis and Treatment
- Non-invasive H. pylori testing: Urea breath test (UBT) — gold standard non-invasive test for active infection; fecal antigen test — high sensitivity and specificity; serology — positive result only confirms past exposure
- Endoscopy: For biopsy (exclude malignancy in gastric ulcers; H. pylori histology); mandatory for gastric ulcers to document healing
- Treatment: Standard triple therapy (PPI + clarithromycin + amoxicillin × 14 days) achieves approximately 80% eradication; rising clarithromycin resistance has reduced efficacy in some regions; quadruple therapy or culture-guided treatment is increasingly preferred
Bowel Conditions
Inflammatory bowel disease, irritable bowel syndrome, and diverticular disease together represent the most common chronic causes of abdominal pain seen in outpatient gastroenterology practice.
Inflammatory Bowel Disease (IBD)
IBD comprises two distinct entities with overlapping features:
- Crohn's disease: Can involve any segment of the gastrointestinal tract from mouth to anus; transmural inflammation; characteristic skip lesions (areas of normal bowel between diseased segments); cobblestone mucosa on endoscopy; terminal ileum is most commonly affected; complications include fistulae (enterocutaneous, enterovaginal, perianal), strictures, and abscesses; vitamin B12 deficiency from terminal ileal disease; surgical resection is common but not curative
- Ulcerative colitis (UC): Limited to the colon and rectum; always begins at the rectum and extends continuously proximally; hallmark symptoms are bloody diarrhea, tenesmus (persistent urge to defecate), and passage of bloody mucus; risk of colorectal cancer increases with disease duration and extent (surveillance colonoscopy is mandatory); fulminant colitis and toxic megacolon are life-threatening complications requiring emergency colectomy
Irritable Bowel Syndrome (IBS)
IBS is the most common gastrointestinal disorder worldwide, affecting 10–15% of the global population. It is defined by the Rome IV criteria: recurrent abdominal pain at least 1 day per week for the past 3 months, associated with two or more of: change in stool frequency, change in stool form (consistency), and association with defecation. Subtypes include IBS with predominant constipation (IBS-C), diarrhea (IBS-D), or mixed pattern (IBS-M). The brain-gut axis dysregulation, visceral hypersensitivity, and altered intestinal motility underlie pathophysiology. IBS should be diagnosed positively based on symptom criteria — not solely by exclusion — in the absence of alarm features. Treatment includes:
- Dietary: Low-FODMAP diet (reduces fermentable oligo-, di-, mono-saccharides and polyols); soluble fiber for IBS-C
- Pharmacological: Rifaximin (non-absorbable antibiotic for IBS-D); linaclotide and lubiprostone (IBS-C); antispasmodics; low-dose antidepressants (TCAs; SNRIs) for pain modulation
- Psychological: Cognitive behavioral therapy (CBT) has strong evidence; gut-directed hypnotherapy; mindfulness-based stress reduction
Diverticular Disease
- Diverticulosis: Outpouchings of colonic mucosa and submucosa through weak points in the bowel wall (where blood vessels penetrate the circular muscle); present in approximately 60% of adults over age 60; predominantly affects the sigmoid colon due to high intraluminal pressure; low-fiber diet is a risk factor; usually asymptomatic
- Acute diverticulitis: Microperforation or macroperforation of a diverticulum → LLQ pain + fever + leukocytosis; CT abdomen/pelvis with contrast is the gold standard (pericolonic fat stranding, thickened bowel wall, abscess, free air); uncomplicated diverticulitis may be managed outpatient with oral antibiotics; complicated diverticulitis (abscess, perforation, fistula, obstruction) requires hospitalization and possible surgical or percutaneous intervention
- Diverticular bleeding: The most common cause of massive lower GI bleeding in adults; characteristically painless; stops spontaneously in approximately 80% of cases; colonoscopy for diagnosis and hemostasis; angioembolization or surgery for refractory bleeding
Functional and Chronic Abdominal Pain
Functional abdominal pain disorders are among the most challenging presentations in medicine. The absence of structural pathology does not mean the pain is imaginary — central sensitization, alterations in pain processing, and biopsychosocial factors produce real, disabling symptoms. Approximately 30–40% of patients presenting with chronic abdominal pain will have a functional disorder as the primary diagnosis.
Pathophysiology of Functional Pain
Central sensitization involves amplification of pain signals at the level of the spinal cord and brain. Visceral hypersensitivity causes patients to perceive normal gut activity (gas, peristalsis) as painful. Psychological comorbidities including anxiety, depression, and post-traumatic stress disorder (PTSD) are common and bidirectional — they both worsen pain and are worsened by chronic pain. Adverse childhood experiences (ACEs) and history of physical or sexual abuse are significantly associated with functional abdominal pain syndromes.
Alarm Features That Must Prompt Organic Workup
Before attributing abdominal pain to a functional cause, the following alarm features must be actively excluded:
- Unintentional weight loss >10% of body weight
- Blood in stool (visible or fecal occult blood test positive)
- Pain that awakens from sleep (particularly nocturnal diarrhea)
- Family history of colorectal cancer (CRC) or inflammatory bowel disease
- Elevated inflammatory markers (CRP, ESR, fecal calprotectin)
- Iron-deficiency anemia or hypoalbuminemia
- Age >50 years with new-onset symptoms; age >40 with new symptoms in high-risk populations
- Rectal bleeding
Diagnostic Workup for Chronic Abdominal Pain
- Basic metabolic panel (CMP) + CBC with differential
- C-reactive protein (CRP) and erythrocyte sedimentation rate (ESR)
- Celiac disease panel: IgA anti-tissue transglutaminase (anti-tTG) antibody + total serum IgA (to exclude IgA deficiency, which would cause a false-negative tTG)
- Fecal calprotectin (distinguishes inflammatory from functional cause; elevated in IBD, infection, malignancy)
- Colonoscopy if alarm features present or age-appropriate cancer screening indicated
- CT abdomen/pelvis for structural evaluation; CT enterography if small bowel Crohn's is suspected
Treatment of Functional Abdominal Pain
- Cognitive behavioral therapy (CBT): Highest level of evidence for IBS and functional abdominal pain; addresses catastrophizing and pain behaviors
- Antidepressants: Tricyclic antidepressants (TCAs) at low dose (e.g., amitriptyline 10–25 mg nightly) reduce visceral hypersensitivity; SNRIs (duloxetine) are an alternative with fewer anticholinergic side effects
- Dietary therapy: Low-FODMAP diet; elimination of identified trigger foods; regular meal timing
- Pelvic floor physical therapy: Particularly effective for patients with pelvic floor dysfunction contributing to abdominal and pelvic pain
- Biofeedback and mindfulness-based interventions: Emerging evidence for pain reduction and quality of life improvement
Diagnostic Workup in the Emergency Setting
The systematic approach to acute abdominal pain in the emergency department begins with hemodynamic assessment and ends with a disposition decision that may range from immediate surgery to reassurance and outpatient follow-up. Speed and accuracy are simultaneously required.
Initial Assessment: ABCs and Hemodynamics
Airway, Breathing, and Circulation must be addressed first. Hypotension, tachycardia, and altered mental status indicate hemodynamic instability and narrow the differential to immediately life-threatening diagnoses: ruptured AAA, septic shock from peritonitis, massive GI hemorrhage, or ruptured ectopic pregnancy. Resuscitation (large-bore IV access, fluid resuscitation, blood products if indicated) and immediate surgical consultation proceed simultaneously with diagnostic evaluation.
History
A structured history using the OPQRST framework (Onset, Provocation/Palliation, Quality, Radiation, Severity, Timing) is essential:
- Onset: Sudden (perforation, AAA rupture, mesenteric ischemia, ovarian torsion) vs. gradual (appendicitis, diverticulitis, IBD exacerbation)
- Location and radiation: RUQ → shoulder (biliary); periumbilical → RLQ (appendicitis); epigastric → back (pancreatitis, AAA); periumbilical (small bowel obstruction)
- Character: Colicky (bowel obstruction, biliary colic, renal colic) vs. constant (peritonitis, ischemia, cholecystitis) vs. burning (peptic ulcer, GERD)
- Associated symptoms: Fever (infection, inflammatory); vomiting (obstruction, pancreatitis, appendicitis); jaundice (biliary, hepatic); hematochezia/melena (GI bleeding); amenorrhea (ectopic pregnancy)
- Relevant history: Prior surgeries (adhesions → SBO); medications (NSAIDs → PUD; anticoagulants → GI bleeding); last normal bowel movement (obstipation → obstruction or severe ileus); last menstrual period and pregnancy status
Physical Examination
Systematic abdominal examination follows inspection → auscultation → percussion → palpation:
- Inspection: Distension (obstruction; ascites); visible peristalsis (obstruction); surgical scars (adhesions); ecchymosis (Grey Turner's = flank; Cullen's = periumbilical = retroperitoneal hemorrhage, severe pancreatitis)
- Auscultation: Absent bowel sounds (ileus; peritonitis; late obstruction); high-pitched "tinkling" sounds (early mechanical obstruction); succussion splash (gastric outlet obstruction)
- Percussion: Tympany (gas-filled loops; obstruction); dullness (fluid, solid mass, organomegaly); percussion tenderness (peritoneal irritation; more sensitive than rebound)
- Palpation: Begin away from the area of maximum pain; assess voluntary guarding (patient can relax on request — protective response) vs. involuntary guarding (cannot relax — parietal peritoneal inflammation = surgical emergency); rigidity; rebound tenderness
Peritoneal Signs — Surgical Emergency
The combination of involuntary guarding + rigidity + rebound tenderness indicates parietal peritoneal involvement and constitutes a surgical emergency. Immediate surgical consultation is required. Do not delay for additional imaging in an unstable patient with clear peritoneal signs.
Laboratory Evaluation
- CBC: Leukocytosis (infection, inflammation); anemia (GI bleeding, hemolysis); thrombocytopenia (sepsis)
- Complete metabolic panel (CMP): Liver enzymes (hepatic, biliary); renal function (renal colic, dehydration from vomiting); electrolytes; glucose (DKA)
- Lipase: Elevated >3× upper limit of normal is diagnostic for acute pancreatitis (amylase is less specific)
- Lactate: Elevated in mesenteric ischemia, bowel strangulation, and septic shock; a critical marker not to omit in severe abdominal pain
- Urinalysis (UA): Hematuria (renal/ureteral colic); WBCs (UTI, pyelonephritis, or contamination from adjacent inflammatory process)
- Urine pregnancy test: Mandatory in all women of childbearing age; do not skip even if the patient reports recent menstruation
- Blood cultures: Obtain before antibiotics in patients with fever, hemodynamic instability, or suspicion of intraabdominal sepsis
Imaging
- Plain abdominal X-ray (KUB): Rapidly identifies free air under the diaphragm (perforation), air-fluid levels (obstruction), sigmoid volvulus ("coffee-bean" sign), and fecal impaction; sensitivity limited but fast and low radiation
- Upright chest X-ray: More sensitive than KUB for free intraperitoneal air (detects as little as 1 mL of free air); always order upright in suspected perforation
- CT abdomen/pelvis with IV contrast: Most informative single study; sensitivity >95% for most acute intraabdominal pathology; diagnoses appendicitis, diverticulitis, pancreatitis, bowel obstruction, mesenteric ischemia, AAA, intraabdominal abscesses; contraindicated in renal failure (use non-contrast CT or alternative imaging)
- Ultrasound: First-line for biliary pathology (gallstones, cholecystitis) and gynecologic emergencies (ovarian torsion, ectopic pregnancy); bedside FAST exam for free fluid (hemoperitoneum); preferred in children and pregnant women; operator-dependent
Key Research Papers
- Salminen P, et al. "Antibiotic Therapy vs Appendectomy for Treatment of Uncomplicated Acute Appendicitis: The APPAC Randomized Clinical Trial." JAMA. 2015;313(23):2340–2348. PMID: 26080338. DOI: 10.1001/jama.2015.6154
- Peery AF, et al. "Burden and Cost of Gastrointestinal, Liver, and Pancreatic Diseases in the United States." Gastroenterology. 2019;156(1):254–272. PMID: 30315778. DOI: 10.1053/j.gastro.2018.08.063
- Drossman DA. "Functional Gastrointestinal Disorders: History, Pathophysiology, Clinical Features, and Rome IV." Gastroenterology. 2016;150(6):1262–1279. PMID: 27144617. DOI: 10.1053/j.gastro.2016.02.032
- Lacy BE, et al. "Bowel Disorders." Gastroenterology. 2016;150(6):1393–1407. PMID: 27144627. DOI: 10.1053/j.gastro.2016.02.031
- Birnbaum BA, Wilson SR. "Appendicitis at the Millennium." Radiology. 2000;215(2):337–348. PMID: 10796905. DOI: 10.1148/radiology.215.2.r00ap24337
- Kwan KY, Nager AL. "Diagnosing Pediatric Appendicitis: Usefulness of Laboratory Markers." Am J Emerg Med. 2010;28(9):1009–1015 — Search PubMed. DOI: 10.1016/j.ajem.2009.06.004
- Strate LL, et al. "Diverticular Disease as a Chronic Illness: Evolving Epidemiologic and Clinical Insights." Am J Gastroenterol. 2016;111(5):654–666 — Search PubMed. DOI: 10.1038/ajg.2016.67
- Lau JY, et al. "Systematic review of the epidemiology of complicated peptic ulcer disease." Aliment Pharmacol Ther. 2011;34(3):303–315 — Search PubMed. DOI: 10.1111/j.1365-2036.2011.04682.x
- Harbrecht BG, Franklin GA. "Management of acute pancreatitis." Am Surg. 2010;76(12):1298–1304 — Search PubMed
- Ng SC, et al. "Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century." Lancet. 2017;390(10114):2769–2778. PMID: 29050646. DOI: 10.1016/S0140-6736(17)32448-0
- Rubano E, et al. "Systematic review: emergency visceral artery revascularization." J Trauma Acute Care Surg. 2013;75(1):102–111. PMID: 23778446. DOI: 10.1097/TA.0b013e318295f7a8
- Ford AC, et al. "Global prevalence of, and risk factors for, uninvestigated dyspepsia." Gut. 2020;69(7):1190–1202 — Search PubMed. DOI: 10.1136/gutjnl-2019-319843
Search PubMed: Abdominal Pain Emergency Diagnosis Acute Abdomen Imaging and Surgery