Pyloric Stenosis (Hypertrophic Pyloric Stenosis)
- Overview and Epidemiology
- Pathophysiology
- Clinical Presentation
- The Classic Electrolyte Derangement
- Diagnosis — Ultrasound and Beyond
- Differential Diagnosis of Infant Vomiting
- Pre-operative Resuscitation
- Ramstedt Pyloromyotomy
- Post-operative Care and Outcomes
- Key Research Papers
- Connections
Overview and Epidemiology
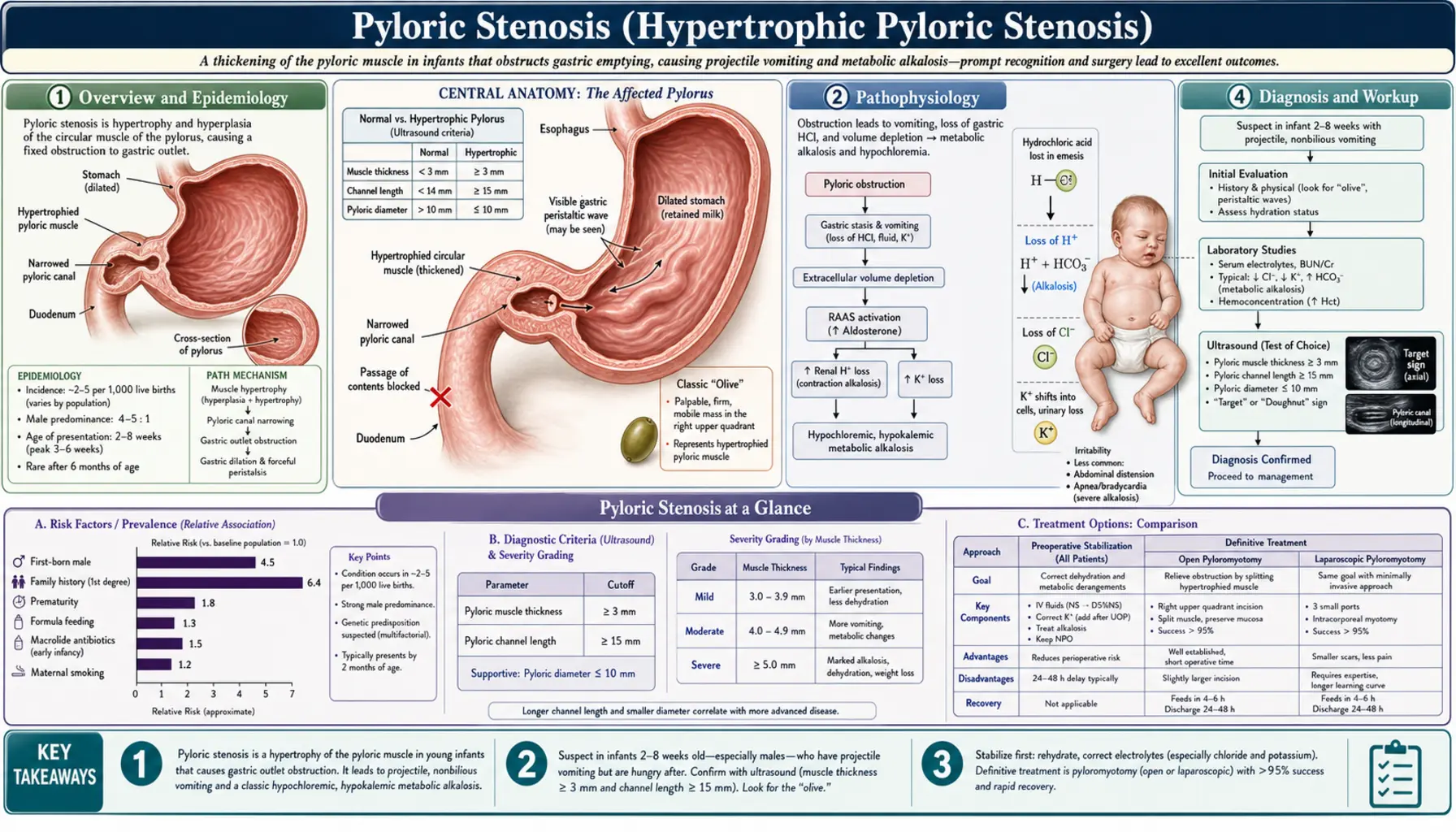
Hypertrophic pyloric stenosis (HPS) is the most common surgical cause of vomiting in infancy and one of the most common conditions requiring surgery in the first few months of life. It occurs when the muscular wall of the pylorus — the short canal connecting the stomach to the duodenum — undergoes progressive hypertrophy, narrowing the outlet until the stomach cannot empty effectively.
Incidence in Western populations is approximately 2–4 per 1,000 live births, though this varies substantially by ethnicity: rates are higher in White Northern European populations and lower in Black and Asian populations. There is a striking 4:1 male predominance, with boys affected far more often than girls. The reasons for this sex bias are incompletely understood but likely involve androgen-dependent effects on pyloric smooth muscle.
The condition presents between 2 and 8 weeks of age (onset before 2 weeks or after 12 weeks is rare). First-born males are at highest risk — first-born males have approximately twice the risk of later-born males. The reason for birth-order effect is unclear; altered gut microbiome from first-time breastfeeding, different feeding practices with first children, and subtle genetic interactions have all been proposed.
Other established risk factors include:
- Family history: if the mother had HPS, her son has a ~20% risk and her daughter ~7%; if the father had HPS, risk is ~5% for a son and ~2.5% for a daughter — confirming multifactorial genetic inheritance
- Macrolide antibiotic exposure: use of erythromycin in the first 2 weeks of life (to treat pertussis prophylaxis or chlamydial conjunctivitis) increases HPS risk approximately 8-fold; azithromycin carries lower but still elevated risk; the mechanism involves the motilin-receptor agonist properties of macrolides, which cause intense pyloric contractions
- Bottle-feeding: historically associated in some studies, though many exclusively breastfed infants develop HPS
Since its first description by Harald Hirschsprung in 1888 and the development of Ramstedt's curative pyloromyotomy in 1912, pyloric stenosis has gone from a frequently fatal condition to one with essentially zero mortality in high-resource settings with prompt diagnosis and appropriate surgical care.
Pathophysiology
The pyloric channel normally measures 2–3 mm in muscle wall thickness and approximately 12–14 mm in length in a newborn. In HPS, the circular and longitudinal muscle layers of the pylorus undergo progressive hypertrophy and hyperplasia, thickening the muscle wall and elongating the canal until it resembles a firm, white, olive-shaped mass. The lumen narrows to a pinhole that cannot pass food.
The trigger for this aberrant muscle growth remains unclear despite decades of research. Current evidence points to an interstitial cell of Cajal (ICC) deficiency. ICCs are the pacemaker cells of the gut that coordinate smooth muscle contractions; they are markedly reduced in the hypertrophied pylorus of HPS. Without normal ICC-mediated relaxation signals, the pyloric muscle remains in a state of persistent partial contraction, and the mechanical stress of peristaltic contractions against this non-relaxing outlet drives further hypertrophy in a self-reinforcing cycle.
Neuronal nitric oxide synthase (nNOS) is another key player. nNOS-expressing neurons in the myenteric plexus normally release nitric oxide to relax smooth muscle. HPS pylori show marked reduction in nNOS neurons. Without nitric oxide-mediated relaxation, pyloric smooth muscle tone is exaggerated. This finding also explains why pharmacological approaches (atropine, which blocks acetylcholine-mediated contraction) have had limited success — the fundamental problem is not excessive excitation but loss of inhibitory relaxation.
Genetic studies have identified several susceptibility loci including regions on chromosomes 11q14-22, MBNL1, and EML4. The condition likely results from the interaction of multiple genes and environmental triggers rather than a single-gene defect. The concordance rate in monozygotic twins is 25–40%, confirming that environmental factors modify genetic risk.
Because the obstruction is at the pylorus (distal to the stomach, before the duodenum), the vomited material is entirely gastric — no bile, no duodenal contents. This is the defining clinical feature: non-bilious vomiting. Any vomiting with bile (green) in an infant suggests a more distal obstruction (malrotation, duodenal atresia) and is a surgical emergency.
Clinical Presentation
The presentation of pyloric stenosis has a classic trajectory that becomes more recognizable once understood. Parents typically describe a baby who was feeding normally for the first few weeks of life, then began vomiting, with the vomiting progressively worsening over 1–2 weeks until it is occurring with every feed.
The cardinal feature is projectile non-bilious vomiting:
- Non-bilious — clear, white, or curdled — never green. The obstruction is proximal to the ampulla of Vater where bile enters the bowel.
- Projectile — forceful, often shooting several feet across the room; this reflects the powerful peristaltic contractions of a hypertrophied stomach attempting to force milk through the narrowed pyloric channel. Not all cases are dramatically projectile early in the course, and parents may initially describe "spit-up" that progressively worsens.
- Post-vomiting hunger — the infant typically feeds eagerly immediately after vomiting ("hungry vomiter"). This distinguishes HPS from other causes of vomiting in infants; a baby who vomits and then does not want to feed suggests a different pathology.
Physical examination findings:
- Visible gastric peristalsis — waves of peristalsis visible through the thin abdominal wall moving from left to right across the upper abdomen. This occurs because the stomach is vigorously contracting against the obstructed pylorus. Elicited by feeding the infant during examination.
- Palpable pyloric mass ("olive") — a firm, smooth, 1.5–2 cm oval mass in the right epigastrium or right upper quadrant, palpated most easily after vomiting when the stomach is empty and the infant is relaxed. This is the hypertrophied pylorus. Requires an experienced examiner; best palpated after a test feed that empties by vomiting. In the ultrasound era, the olive is sought less aggressively but remains a useful finding when present.
- Signs of dehydration: sunken fontanelle, dry mucous membranes, decreased skin turgor, decreased wet diapers
- Weight loss or failure to gain weight appropriate to age
- Jaundice — approximately 5% of infants with HPS develop conjugated hyperbilirubinemia ("icteropyloric syndrome"), attributed to caloric deprivation reducing hepatic glucuronosyltransferase activity. It resolves promptly after successful surgery.
The Classic Electrolyte Derangement
The metabolic consequence of repeated vomiting in HPS is one of the most elegant examples of physiology in clinical medicine: hypochloremic hypokalemic metabolic alkalosis. Understanding it mechanistically (not by rote memorization) allows confident prediction and management.
Step 1 — Losing gastric contents. Every vomit ejects gastric juice, which is rich in hydrochloric acid (HCl). Each molecule of HCl lost removes one H⁺ and one Cl⁻ from the body. Serum chloride falls. The loss of H⁺ means less acid in the blood — bicarbonate accumulates and pH rises: metabolic alkalosis.
Step 2 — The kidney's initial response. As metabolic alkalosis develops, the kidney attempts to correct the pH by excreting bicarbonate. Bicarbonate exits in the urine as NaHCO₃, pulling sodium with it. Urine is alkaline at this stage.
Step 3 — Volume depletion takes priority. As vomiting continues, the infant becomes volume-depleted. The kidney now has a competing priority: preserve sodium and water (via the renin-angiotensin-aldosterone system, RAAS). Aldosterone secretion rises, directing the kidney to retain sodium. But aldosterone drives a Na⁺/K⁺ exchange in the collecting duct — to retain one Na⁺, the kidney excretes one K⁺. Hypokalemia develops.
Step 4 — Paradoxical aciduria. As potassium becomes depleted, the Na⁺/K⁺ exchange in the collecting duct cannot be sustained. The kidney shifts to a Na⁺/H⁺ exchange instead — excreting H⁺ to preserve Na⁺, even though the body is alkalotic. The urine becomes acidic despite systemic alkalosis: paradoxical aciduria. This is a late finding indicating severe depletion and immediate need for fluid resuscitation.
Summary of the typical blood gas and electrolyte pattern in HPS:
| Parameter | Direction | Typical value (moderate depletion) |
|---|---|---|
| pH | High | 7.50–7.60 |
| Bicarbonate (HCO₃) | High | 28–40 mEq/L |
| Chloride (Cl⁻) | Low | 85–95 mEq/L (normal 98–106) |
| Potassium (K⁺) | Low | 3.0–3.5 mEq/L |
| Sodium (Na⁺) | Low-normal | 130–140 mEq/L |
| Urine pH | Paradoxically low | <6.0 in severe depletion |
The key clinical principle: this derangement is not a medical emergency — it is a surgical emergency that must wait until the metabolic derangement is corrected. Anesthesia in the setting of severe alkalosis carries serious risks (cardiac arrhythmias, impaired ventilator weaning, laryngospasm at extubation). Safe anesthesia requires a bicarbonate below approximately 26–30 mEq/L, normochloremia, and normokalemia.
Diagnosis — Ultrasound and Beyond
Ultrasound has replaced clinical examination as the primary diagnostic tool since the 1980s and is now considered the gold-standard investigation for suspected HPS.
Ultrasound criteria for HPS (Teele and Share, validated across multiple studies):
- Pyloric muscle thickness >4 mm — the most sensitive individual criterion; measures the echogenic circular muscle layer on transverse view
- Pyloric channel length >17 mm — measured in longitudinal section from gastric antrum to duodenum
- Pyloric transverse diameter >13–14 mm
When both muscle thickness >4 mm and channel length >17 mm are met, ultrasound has sensitivity >97% and specificity approaching 100% for HPS. Findings are confirmed by observing absence of flow through the pyloric channel during real-time scanning: the stomach fills, contracts vigorously, but gastric contents cannot pass into the duodenum.
What ultrasound cannot always tell: In the first 2–3 weeks of the clinical course, the pylorus may not yet meet full criteria even if HPS is the underlying diagnosis. A borderline ultrasound in a child with classic symptoms warrants a repeat study in 24–48 hours or discussion with a pediatric surgeon.
Upper GI contrast series (barium/water-soluble contrast): Largely replaced by ultrasound but still used in some centers or when ultrasound is equivocal. Classic findings include the "string sign" (thin line of contrast squeezed through the elongated pyloric channel), the "double-track sign" (parallel tracks of contrast separated by the hypertrophied pyloric ridges), and the "shoulder sign" (pyloric muscle bulging into the gastric antrum).
Investigations at presentation should also include: electrolytes (sodium, potassium, chloride, bicarbonate), blood gas (venous acceptable), serum glucose, full blood count (assess for anemia), and urinalysis.
Differential Diagnosis of Infant Vomiting
Non-bilious vomiting in a young infant has a broad differential. The combination of age, vomiting character, clinical findings, and ultrasound differentiates HPS from alternatives.
| Condition | Age | Vomit character | Key differentiating features |
|---|---|---|---|
| Pyloric stenosis (HPS) | 2–8 weeks | Non-bilious, projectile | Hungry after vomiting; palpable olive; US confirms |
| Gastro-oesophageal reflux (GOR) | Any infant age | Non-bilious, effortless ("happy spitter") | Not projectile; not hungry after; no weight loss; resolves with positioning/feeds |
| Overfeeding | Any infant age | Non-bilious | Excessive feed volumes; no distress; thriving; resolve with volume reduction |
| Malrotation with midgut volvulus | Any age (often <1 month) | Bilious | SURGICAL EMERGENCY; bile = red flag; abdominal distension; shock |
| Duodenal atresia / web | Newborn period | Bilious (post-ampullary) or non-bilious (pre-ampullary) | Often diagnosed antenatally; "double bubble" on X-ray |
| Pyloric atresia | Newborn | Non-bilious | Rare; gasless abdomen; complete obstruction from birth |
| Congenital adrenal hyperplasia (salt-wasting) | 2–4 weeks | Non-bilious | Hyponatremia + hyperkalemia (opposite of HPS); ambiguous genitalia in girls; adrenal crisis |
| Pyloric spasm | 2–8 weeks | Non-bilious | US shows normal pyloric dimensions but functional spasm; may respond to atropine |
| Sepsis / meningitis | Any neonatal age | Non-bilious | Ill-appearing; temperature instability; bulging fontanelle; CSF abnormal |
Critical rule: bilious vomiting in any infant is a surgical emergency until proven otherwise. Malrotation with midgut volvulus can infarct the entire midgut in hours. An infant with bilious (green) vomiting requires urgent surgical consultation regardless of how well the infant appears.
Pre-operative Resuscitation
Pyloric stenosis is not an emergency operation. There is no benefit to rushing to theater before the metabolic derangement is corrected; significant harm can result from anesthetizing a severely alkalotic, hypokalemic infant. The appropriate mindset is: stabilize, correct, then operate.
Fluid resuscitation protocol:
- Stop oral feeds — pass a nasogastric tube and aspirate any residual gastric contents to prevent aspiration. Leave the tube on free drainage to decompress the stomach.
- Initial bolus — for signs of haemodynamic compromise (poor perfusion, tachycardia): 10–20 mL/kg isotonic saline (0.9% NaCl) over 30–60 minutes. This expands circulating volume. Most infants with HPS are volume-depleted but not in shock.
- Maintenance and replacement fluids — after initial resuscitation, run 0.45% NaCl + 5% dextrose + 20–40 mEq/L KCl at 1.5 times maintenance. The chloride load corrects the hypochloremia and allows the kidney to excrete bicarbonate (once chloride is available, the kidney can finally reabsorb chloride instead of bicarbonate). Potassium supplementation corrects hypokalemia.
- Monitoring — measure electrolytes every 4–6 hours; repeat blood gas. The biochemical targets before anesthesia are:
- Serum bicarbonate <30 mEq/L (ideally <26)
- Chloride >95 mEq/L
- Potassium >3.5 mEq/L
- Adequate urine output (>1 mL/kg/hr)
Most infants reach these targets within 24–48 hours of appropriate resuscitation. Severe derangements may require 72 hours. There is no value in operating sooner.
Ramstedt Pyloromyotomy
The Ramstedt pyloromyotomy, first performed by Conrad Ramstedt in 1912, remains the definitive curative treatment for HPS more than 110 years after its introduction. The operation is elegant in its simplicity: divide the hypertrophied pyloric muscle longitudinally without entering the mucosa, allowing the pyloric channel to spring open.
Surgical technique: Under general anesthesia, the pylorus is delivered through a right upper quadrant transverse incision (open approach) or through 3 laparoscopic ports (laparoscopic approach). The hypertrophied pyloric muscle is incised longitudinally with a knife or diathermy from the gastric antrum to the duodenum. The incision is deepened through the full thickness of the muscle, and the fibers are bluntly separated to allow the pyloric mucosa to bulge upward through the gap. A successful myotomy shows the mucosa clearly visible in the base of the divided muscle, with no resistance to spreading, and inflation of the stomach with air via nasogastric tube confirms no mucosal perforation.
Laparoscopic vs open pyloromyotomy: Multiple randomized controlled trials and meta-analyses have compared the two approaches. Laparoscopic pyloromyotomy offers:
- Smaller incisions and improved cosmesis
- Faster return to full feeds (by approximately 4–8 hours) and shorter hospital stay (by approximately half a day) in some studies
- Equivalent safety profile
In experienced hands, both approaches have essentially identical outcomes and complication rates. The choice depends on surgeon expertise — a laparoscopic pyloromyotomy in inexperienced hands has a higher mucosal perforation rate than an open procedure by a skilled surgeon. The operation should be performed by a pediatric surgeon experienced in the procedure.
Complications of pyloromyotomy (overall complication rate <5% in experienced centers):
- Mucosal perforation (0.5–2%) — most common serious complication; recognized and repaired immediately; requires a second myotomy site on the anterior wall of the pylorus
- Incomplete myotomy (<1%) — insufficient muscle division leaving residual obstruction; requires repeat operation if vomiting persists beyond 48–72 hours post-operatively
- Wound infection — more common with open approach
Medical (non-surgical) alternative: Oral atropine sulfate has been used in Japan and some European centers as an alternative to surgery, particularly in infants with cardiac contraindications to anesthesia. Atropine relaxes pyloric smooth muscle by blocking muscarinic acetylcholine receptors. A 2021 RCT (the BÉNI study, France) showed oral atropine was non-inferior to surgery in achieving symptom resolution, with 87% of atropine-treated infants symptom-free at 3 months vs 96% for surgery. However, atropine requires 3 weeks of treatment, prolonged hospitalization in some protocols, and a significantly longer time to cure. It is not standard of care in North American or UK practice but represents a valid option for selected patients.
Post-operative Care and Outcomes
Recovery from Ramstedt pyloromyotomy is rapid. The pyloric muscle heals over 2–4 weeks, but after successful surgery the pyloric channel is permanently widened and the condition does not recur.
Post-operative feeding: Most protocols allow small feeds of breast milk or formula to begin 4–6 hours after surgery, with volumes progressively increased over 24 hours to full feeds. Some centers use an ad lib demand-feeding approach from 3–4 hours post-op. Post-operative vomiting is common in the first 24–48 hours and should not trigger alarm — the stomach has adapted to persistent obstruction and takes time to normalize its motility and size. Parents should be warned that some vomiting in the first few days after surgery is normal and does not indicate a complication.
Hospital stay: Most infants are discharged 24–48 hours after surgery, once tolerating full feeds. Some centers achieve same-day or next-day discharge in uncomplicated cases.
Breastfeeding: Mothers should be strongly supported to continue breastfeeding. They should be counseled to pump during the nil-by-mouth period and the initial restricted-feed phase to maintain milk supply. Breastfeeding success rates are high after HPS surgery when proactively supported.
Long-term outcomes are excellent. There is no increased risk of pyloric pathology in adulthood. Gastrointestinal function is normal. Growth and development proceed normally after recovery from the episode of acute illness. Multiple long-term follow-up studies (up to 45 years) have found no increased rates of peptic ulcer disease, gastro-oesophageal reflux, or functional gastrointestinal disorders compared to the general population.
The mortality rate for HPS in high-resource settings is effectively zero when diagnosed and managed appropriately. Deaths, when they occur, result from delayed diagnosis leading to severe malnutrition and electrolyte derangement or from aspiration during anesthesia — both preventable with timely recognition and adequate pre-operative resuscitation.
Key Research Papers
- Search PubMed — Comprehensive surgical review covering incidence, pathophysiology, diagnosis, operative technique, and outcomes including comparative data for open vs laparoscopic approaches.
- Search PubMed — Reference establishing the definitive ultrasound criteria for HPS (muscle thickness >4mm, channel length >17mm) that remain in universal use.
- Search PubMed — Meta-analysis of RCTs and prospective studies comparing laparoscopic vs open pyloromyotomy; demonstrated equivalent complication rates with shorter hospital stay for laparoscopic approach.
- Search PubMed — Review of imaging strategies including ultrasound and upper GI contrast series; discusses diagnostic accuracy and practical approach to equivocal ultrasounds.
- Search PubMed — Population-based Danish cohort study quantifying familial recurrence rates; established the pattern of sex-specific inheritance and first-born male predominance.
- Search PubMed — Key study linking neonatal erythromycin exposure to 8-fold increase in HPS risk, with important implications for antibiotic prescribing in neonates.
- Search PubMed — Early experience report comparing laparoscopic to open technique demonstrating feasibility and safety of laparoscopic approach in experienced hands.
- Jacobsen BH et al., 2017 — Medical vs. surgical treatment of infantile hypertrophic pyloric stenosis — Journal of Pediatric Gastroenterology and Nutrition — PMID: 28902019 — Systematic review of atropine medical treatment evidence; established efficacy data and context for the surgical vs. medical debate.
- Search PubMed — Up-to-date narrative review covering all aspects of HPS management including emerging evidence for oral atropine and post-operative feeding protocols.
- Search PubMed — Outcomes analysis confirming near-zero mortality with contemporary surgical management and identifying pre-operative optimization as the key safety determinant.
- Search PubMed — Review of non-surgical (atropine) approaches with critical assessment of evidence quality; places the BÉNI trial results in clinical context.
- Search PubMed — Demonstrated that ultrasound is superior to physical examination in confirming HPS; only 59% of confirmed HPS cases had a palpable olive, validating ultrasound as first-line investigation.
Connections
- Pediatrics
- Neonatal Jaundice
- Febrile Seizures
- Intussusception
- Kawasaki Disease
- Croup
- Gastroenterology
- Potassium