Choledocholithiasis
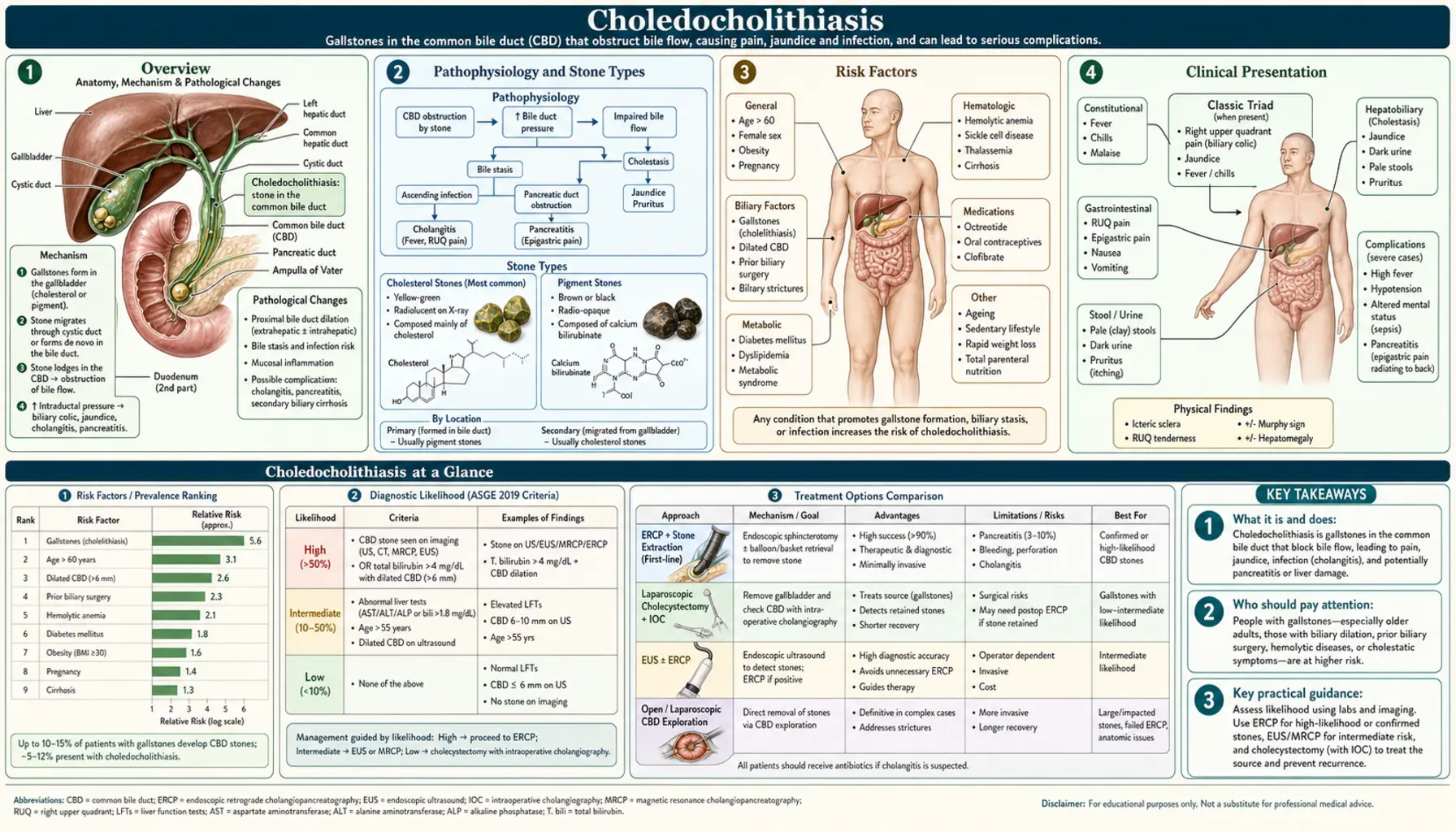
Choledocholithiasis — stones lodged in the common bile duct — complicates 10 to 20 percent of all gallstone disease and can escalate without warning from silent obstruction to life-threatening ascending cholangitis or acute pancreatitis. Understanding how these stones form, how to find them, and how to remove them is central to biliary medicine.
Table of Contents
- Overview
- Pathophysiology and Stone Types
- Risk Factors
- Clinical Presentation
- Charcot's Triad and Reynolds' Pentad
- Diagnosis
- ERCP — Endoscopic Retrograde Cholangiopancreatography
- Surgical and Alternative Management
- Complications
- Research Papers
- Connections
- Featured Videos
Overview
Choledocholithiasis is the presence of one or more stones in the common bile duct (CBD). It is found in roughly 10 to 20 percent of patients who have gallstones. Stones in the CBD fall into two categories based on where they originate:
- Secondary stones (the most common type in Western populations): cholesterol or black pigment stones that form first in the gallbladder and then migrate through the cystic duct into the CBD.
- Primary stones: brown pigment stones that form de novo inside the bile ducts, usually due to a combination of bacterial infection and biliary stasis.
Clinically, choledocholithiasis spans a wide spectrum. Some patients have CBD stones found incidentally on imaging with no symptoms at all. Others present with classic biliary colic, obstructive jaundice (dark urine, pale stools, yellow skin and eyes), or the feared triad of pain, fever, and jaundice that signals ascending cholangitis. When a stone impacts at the ampulla of Vater, it can trigger acute pancreatitis by blocking pancreatic duct outflow.
Treatment in the vast majority of cases is endoscopic: ERCP with sphincterotomy and stone extraction achieves clearance in over 90 percent of cases. Definitive management also requires addressing the gallbladder source — laparoscopic cholecystectomy is recommended to prevent recurrence.
Pathophysiology and Stone Types
Understanding why stones form in the CBD requires tracing two distinct pathways: migration from the gallbladder and in-situ formation within the duct itself.
Secondary Stones (Migratory)
The majority of CBD stones in Western patients are secondary — they originate in the gallbladder as either cholesterol stones (the most prevalent type, formed when bile becomes supersaturated with cholesterol relative to bile salts and lecithin) or black pigment stones (calcium bilirubinate aggregates associated with hemolytic conditions and liver cirrhosis). Once formed, stones can slip through the cystic duct into the CBD, particularly during episodes of biliary colic when vigorous gallbladder contraction is triggered by cholecystokinin (CCK) release after a fatty meal.
Primary Stones (De Novo in Duct)
Primary CBD stones are brown pigment stones composed of calcium bilirubinate and calcium soaps of fatty acids. They form directly in the bile ducts under two conditions acting in concert:
- Bacterial infection: Organisms such as Escherichia coli produce beta-glucuronidase, an enzyme that deconjugates bilirubin glucuronide into free unconjugated bilirubin. This insoluble form precipitates with calcium to form calcium bilirubinate crystals. Bacteria also produce phospholipases that release fatty acids from lecithin, generating additional calcium soaps.
- Biliary stasis: Slow or obstructed bile flow (from strictures, anatomical variants, or sphincter of Oddi dysfunction) allows time for crystals to aggregate and grow into stones.
Primary stones are far more common in East and Southeast Asian populations, where liver flukes (Clonorchis sinensis, Opisthorchis species) cause chronic biliary infection and ductal damage — a condition sometimes called recurrent pyogenic cholangitis or Oriental cholangiohepatitis.
Consequences of CBD Obstruction
Once a stone obstructs the CBD, a cascade follows:
- Bile cannot drain into the duodenum → conjugated bilirubin (already processed by hepatocytes) backs up into the bloodstream → jaundice, dark urine (bilirubinuria), and acholic (pale, clay-colored) stools.
- Stasis proximal to the obstruction invites ascending bacterial colonization → cholangitis.
- Impaction at the ampulla of Vater blocks the shared pancreatic duct channel → premature activation of pancreatic enzymes → acute pancreatitis.
- Chronic obstruction increases back-pressure on hepatocytes → secondary biliary cirrhosis over months to years.
The CBD is normally less than 6 mm in diameter on ultrasound (up to 8 mm is acceptable in patients who have had a prior cholecystectomy, where mild duct dilation is a known normal variant). Obstruction causes measurable dilation that serves as an important indirect imaging sign when the stone itself is not directly visualized.
Risk Factors
Risk factors for choledocholithiasis map closely onto risk factors for gallstones — since the vast majority of CBD stones originate there — plus additional factors that promote primary duct stone formation or stone migration.
- Gallstones (cholelithiasis): The dominant risk factor for secondary CBD stones. Any patient with symptomatic gallstones should be evaluated for concurrent CBD stones before or during cholecystectomy.
- Advancing age: Bile composition becomes more lithogenic with age; sphincter of Oddi relaxation in older patients may facilitate migration.
- Biliary infections: Promote primary brown pigment stone formation via bacterial beta-glucuronidase activity.
- Biliary strictures: Postoperative strictures (after cholecystectomy, hepatobiliary surgery, or liver transplant), primary sclerosing cholangitis (PSC), and other stricturing conditions create focal stasis zones where primary stones can form or secondary stones can lodge.
- Hemolytic conditions: Sickle cell disease, hereditary spherocytosis, and thalassemia increase unconjugated bilirubin load, driving black pigment stone formation in both the gallbladder and ducts.
- Liver fluke infestation: Clonorchis sinensis and related flukes, endemic in parts of East and Southeast Asia, inhabit the biliary tree, cause chronic inflammation, and strongly predispose to primary duct stones and recurrent cholangitis.
- Prior biliary procedures: Previous ERCP or surgical biliary instrumentation can inadvertently push small gallbladder stones into the CBD. Biliary-enteric anastomoses (choledochojejunostomy, hepaticojejunostomy) allow reflux of intestinal bacteria, increasing primary stone risk.
- Obesity and rapid weight loss: These increase cholesterol secretion into bile, promoting stone formation in the gallbladder and raising the risk of CBD involvement.
Clinical Presentation
The clinical picture of choledocholithiasis ranges from no symptoms at all to a surgical emergency, depending on whether the stone causes complete obstruction and whether infection supervenes.
Asymptomatic Discovery
A significant proportion of CBD stones — particularly small ones — are found incidentally during imaging for other purposes (abdominal ultrasound, CT, or MRCP) or detected intraoperatively during laparoscopic cholecystectomy. These patients have no pain, no jaundice, and normal liver enzymes. Even asymptomatic CBD stones are generally treated, because the risk of future complications (cholangitis, pancreatitis) outweighs the procedural risk of ERCP.
Biliary Colic
When a stone partially or intermittently obstructs the CBD, patients experience biliary colic: a steady (not truly colicky in the alternating-crampy sense) epigastric or right upper quadrant (RUQ) pain that builds over 15 to 30 minutes, plateaus at high intensity, then gradually resolves over 30 minutes to 6 hours. Pain often radiates to the right shoulder or subscapular area (referred via the phrenic nerve from diaphragmatic peritoneum). Episodes are classically triggered postprandially, when CCK-driven gallbladder and biliary contraction forces a stone against the obstructed duct.
Obstructive Jaundice
Complete or near-complete CBD obstruction impairs bilirubin excretion. The clinical syndrome of obstructive (conjugated, direct) hyperbilirubinemia includes:
- Jaundice: yellow discoloration first visible in the sclerae (icterus), then skin; noticeable when total bilirubin exceeds roughly 2 to 3 mg/dL.
- Dark urine: conjugated bilirubin is water-soluble and excreted in urine, giving it a dark amber or tea-colored appearance (bilirubinuria). A simple dipstick test will show bilirubin in the urine.
- Pale or acholic stools: normally, conjugated bilirubin excreted into the gut is converted by intestinal bacteria to urobilinogen and stercobilin (which gives stool its brown color). Obstruction prevents this — stools become clay-colored or pale gray.
- Pruritus: bile salts deposited in skin cause intense itching, often worse at night and on the palms and soles.
Nausea and Vomiting
Nausea and vomiting accompany acute episodes and are especially prominent when associated with pancreatitis or cholangitis.
Fever and Rigors
Fever — particularly with shaking chills (rigors) — signals that infection has superimposed on the obstruction (ascending cholangitis). This is the most alarming symptom in CBD stone disease and demands urgent evaluation and intervention.
Charcot's Triad and Reynolds' Pentad
Two classic clinical constellations frame the severity assessment of cholangitis complicating CBD stones:
Charcot's Triad (1877)
Described by Jean-Martin Charcot, this triad combines:
- Right upper quadrant or epigastric pain
- Jaundice (obstructive)
- Fever with rigors
This triad is highly specific for ascending cholangitis when all three elements are present, but it appears in only 50 to 70 percent of patients with confirmed cholangitis — many patients, particularly the elderly or immunocompromised, present with fewer or atypical features. The absence of Charcot's triad does not exclude cholangitis.
Reynolds' Pentad
Benedikt Reynolds (1959) extended Charcot's triad with two additional findings that define severe, suppurative (pus-forming) cholangitis:
- RUQ pain
- Jaundice
- Fever
- Altered mental status (confusion, lethargy, obtundation)
- Septic shock (hypotension, tachycardia, end-organ hypoperfusion)
Reynolds' pentad signals purulent bile under high pressure within an obstructed biliary system — a true surgical and endoscopic emergency. Mortality exceeds 50 percent without urgent biliary decompression. When this constellation is recognized, the patient requires simultaneous resuscitation (IV fluids, broad-spectrum antibiotics, vasopressors if needed) and urgent ERCP within hours, not days.
Diagnosis
Diagnosis of choledocholithiasis combines laboratory assessment of hepatobiliary injury, imaging to detect ductal dilation or direct stone visualization, and procedural confirmation when intervention is planned.
Laboratory Findings
- Elevated direct (conjugated) bilirubin: the hallmark of biliary obstruction. Total bilirubin can range from mildly elevated (2 to 5 mg/dL) to severely elevated (>20 mg/dL) depending on completeness of obstruction.
- Elevated alkaline phosphatase (ALP) and gamma-glutamyl transferase (GGT): the classic cholestatic enzyme pattern. ALP may be 3 to 10 times the upper limit of normal; GGT elevation confirms a biliary (not bone) source of ALP rise.
- Elevated ALT and AST: in prolonged obstruction, back-pressure on hepatocytes causes transaminase release. Values may reach several hundred units per liter, mimicking hepatitis; they typically normalize rapidly after biliary decompression.
- Leukocytosis: elevated white cell count with left shift (band neutrophils) indicates superimposed bacterial infection (cholangitis).
- Elevated amylase and lipase: when a CBD stone has impacted at the ampulla of Vater and triggered gallstone pancreatitis. Lipase elevation >3 times normal is the more sensitive and specific marker.
- Coagulation abnormalities: prolonged prothrombin time (PT) can occur in severe or prolonged obstruction, since fat-soluble vitamin K absorption requires bile acids. Parenteral vitamin K may be required before invasive procedures.
Abdominal Ultrasound
Ultrasound is the first-line imaging investigation — it is available, inexpensive, radiation-free, and highly sensitive for CBD dilation (>6 mm). However, it directly visualizes CBD stones in only 50 to 80 percent of cases: distal CBD stones are often obscured by overlying duodenal gas, and small stones (<5 mm) may be missed. A dilated CBD in the correct clinical context strongly suggests obstruction even when a stone is not directly seen.
MRCP (Magnetic Resonance Cholangiopancreatography)
MRCP is the gold-standard non-invasive imaging study for suspected CBD stones. It provides high-resolution three-dimensional images of the biliary tree and pancreatic duct without radiation or contrast injection. Sensitivity for CBD stones is 90 to 95 percent and specificity is approximately 97 percent. MRCP is the preferred investigation when the diagnosis is uncertain (intermediate pre-test probability), when anatomy is complex (prior biliary surgery, strictures), or when ERCP is being considered and the clinician wants to map the biliary tree first to avoid an unnecessary therapeutic procedure. The main limitations are availability, contraindication in patients with incompatible metallic implants (certain pacemakers, cochlear implants), and reduced sensitivity for very small stones (<3 mm).
Endoscopic Ultrasound (EUS)
EUS achieves sensitivity of 89 to 94 percent for CBD stones — comparable to MRCP — by placing an ultrasound transducer within the duodenum, very close to the distal CBD, eliminating the gas-interference problem of transabdominal ultrasound. EUS is preferred when MRCP is contraindicated or unavailable, and it has the advantage that if a stone is confirmed, the endoscopist can proceed directly to ERCP in the same sitting.
CT Scan
CT is less sensitive than MRCP or EUS for CBD stones (approximately 75 percent overall, worse for small or non-calcified stones). It plays a secondary role — useful for detecting complications (periductal inflammation, hepatic abscess, air in the biliary tree suggesting emphysematous cholangitis) or when other diagnoses (pancreatic mass, portal hypertension) are under consideration.
ERCP (Diagnostic Component)
ERCP combines endoscopy with fluoroscopic contrast cholangiography to directly image the biliary tree. Because it carries procedural risk (post-ERCP pancreatitis in 2 to 7 percent), ERCP is now reserved for cases where intervention is anticipated — that is, when pre-procedural imaging (MRCP, EUS) has confirmed or strongly suggested CBD stones. "Diagnostic-only" ERCP has been largely replaced by MRCP and EUS.
Risk Stratification Before ERCP
Several societies (ASGE, ESGE) recommend risk-stratifying patients to guide whether ERCP, MRCP/EUS, or intraoperative cholangiogram is appropriate:
- High probability of CBD stone (ERCP appropriate without prior MRCP): CBD stone visualized on ultrasound, or total bilirubin >4 mg/dL + CBD dilation on ultrasound, or clinical cholangitis.
- Intermediate probability (perform MRCP or EUS first): any other bilirubin elevation with or without CBD dilation, abnormal liver enzymes with risk factors.
- Low probability (no further CBD workup needed): normal bilirubin, normal liver enzymes, no CBD dilation.
ERCP — Endoscopic Retrograde Cholangiopancreatography
ERCP is the primary treatment modality for CBD stones, achieving complete stone clearance in more than 90 percent of cases when performed by experienced endoscopists.
How ERCP Is Performed
The patient receives conscious sedation or general anesthesia. A side-viewing duodenoscope is passed orally through the esophagus, stomach, and into the second part of the duodenum, where the ampulla of Vater is identified. A thin catheter is passed through the instrument channel and cannulated into the CBD (selective biliary cannulation). Fluoroscopic contrast injection produces a cholangiogram — a real-time X-ray map of the biliary tree confirming stone location, number, and size.
Sphincterotomy (also called papillotomy) follows: an electrocautery wire is used to cut through the sphincter of Oddi, widening the biliary orifice. This allows stones to be extracted with a balloon catheter (inflated distal to the stone, then pulled proximally) or a Dormia basket (a wire-loop device that captures stones mechanically).
Management of Large Stones
Stones larger than 15 mm often cannot be extracted intact through even a generous sphincterotomy. These require fragmentation first:
- Mechanical lithotripsy: the stone is captured in a reinforced metal basket and crushed using a handle-mounted mechanical crank — the oldest and still widely used technique.
- Electrohydraulic lithotripsy (EHL): a spark-gap probe generates shock waves directly against the stone surface under direct cholangioscopic visualization (SpyGlass system).
- Laser lithotripsy: pulsed-dye or holmium laser energy fragments stones under direct visual guidance; high success rate even for very hard stones.
Timing of ERCP
- Urgent (<24 hours): cholangitis with organ dysfunction (septic shock, altered mental status, acute kidney injury) — biliary decompression is life-saving and takes priority over everything else.
- Early (<72 hours): stable cholangitis (Charcot's triad without organ dysfunction), or gallstone pancreatitis with concurrent cholangitis or biliary obstruction.
- Elective: asymptomatic or incidentally found CBD stones; symptomatic stones without cholangitis or pancreatitis.
Note: routine early ERCP (<24 hours) for mild gallstone pancreatitis without cholangitis or persistent biliary obstruction does NOT improve outcomes — this is a common clinical misconception. ERCP in uncomplicated pancreatitis adds procedural risk without benefit.
Preventing Post-ERCP Pancreatitis
Post-ERCP pancreatitis (PEP) is the most common serious complication, occurring in 2 to 7 percent of cases overall and up to 15 to 20 percent in high-risk patients (young women, sphincter of Oddi dysfunction, prior PEP). Two evidence-based preventive strategies are now standard of care:
- Rectal indomethacin (100 mg suppository immediately post-procedure): a landmark 2012 New England Journal of Medicine randomized trial (Elmunzer et al., PMID 22494121) demonstrated a 46 percent relative risk reduction in PEP with rectal indomethacin vs. placebo. This is now universally recommended in all patients undergoing ERCP unless contraindicated.
- Prophylactic pancreatic duct stent placement: in high-risk cases (difficult cannulation, pancreatic sphincterotomy, sphincter of Oddi dysfunction type I or II), a small plastic stent is placed into the pancreatic duct to maintain outflow and reduce edema-driven obstruction. The stent is removed endoscopically 1 to 2 weeks later.
ERCP Complications
- Post-ERCP pancreatitis: 2 to 7 percent (most common; usually mild)
- Hemorrhage: 0.3 to 2 percent (post-sphincterotomy; usually self-limited or managed endoscopically)
- Perforation: 0.3 to 1 percent (retroperitoneal perforation from sphincterotomy; often managed conservatively)
- Cholangitis: approximately 1 percent (ascending infection if incomplete drainage; prevented by complete stone clearance and bile duct drainage)
- Contrast reactions: rare with modern iso-osmolar contrast agents
Surgical and Alternative Management
While ERCP is first-line for CBD stone clearance, surgical and radiological alternatives exist — important when ERCP fails, when anatomy precludes standard endoscopic access, or when a single-stage approach during cholecystectomy is preferred.
Laparoscopic Common Bile Duct Exploration (LCBDE)
LCBDE allows the surgeon to clear CBD stones at the same time as cholecystectomy in a single anesthetic event, avoiding the need for a separate ERCP. Access to the CBD is achieved either via a transcystic approach (through the cystic duct) for smaller stones, or via direct choledochotomy (incision into the CBD wall) for larger or more numerous stones. Success rates approach 85 to 90 percent in experienced hands. A randomized trial (Rogers et al., PMID 20083750) found no significant difference in outcomes between LC + LCBDE versus preoperative ERCP + LC. The main limitation is that LCBDE requires specialized laparoscopic biliary surgery training and is not universally available.
Open CBD Exploration
Open surgery is now reserved for cases in which laparoscopic approaches fail or conversion is necessary, or for complex scenarios such as massive stone burden, biliary stricture repair, or concurrent hepatic surgery. It involves direct choledochotomy, stone clearance under direct vision, and usually T-tube drainage of the CBD for several weeks postoperatively.
Percutaneous Transhepatic Cholangiography (PTC)
PTC is a radiological (interventional radiology) approach in which a needle is passed percutaneously through the liver under imaging guidance to access an intrahepatic bile duct. A wire and catheter are advanced through the liver into the CBD, allowing biliary drainage and, ultimately, stone extraction via the percutaneous tract. PTC is indicated when ERCP is not technically feasible:
- Altered surgical anatomy (Billroth II gastrectomy, Roux-en-Y reconstruction) making endoscopic access to the papilla impossible or hazardous
- Duodenal obstruction preventing scope advancement
- Failed ERCP cannulation despite expert attempts
Extracorporeal Shock Wave Lithotripsy (ESWL)
ESWL uses focused external shock waves to fragment stones without endoscopic access. It is now rarely used for CBD stones — reserved for patients who have failed ERCP-based lithotripsy and are not surgical candidates, or for recurrent large stones in the setting of biliary strictures where repeated endoscopic procedures are not feasible.
Timing of Cholecystectomy After ERCP
Removing CBD stones endoscopically without subsequently removing the gallbladder leaves the stone source in place. Recurrent CBD stone episodes occur in 10 to 20 percent of patients with the gallbladder intact. Current guidelines recommend elective laparoscopic cholecystectomy either during the same hospitalization (if the patient is fit for surgery) or within 2 to 6 weeks of ERCP. Indefinite delay significantly increases the risk of recurrent biliary events.
Complications
Untreated or delayed-treatment choledocholithiasis carries serious complication risk. Recognizing these early determines outcome.
Ascending Cholangitis
Bacterial infection superimposed on biliary obstruction is the most common life-threatening complication. Organisms ascend from the duodenum or enter via the portal circulation. The commonest causative bacteria are gram-negative enteric organisms: E. coli, Klebsiella, Enterobacter, and Enterococcus. Anaerobes (Bacteroides, Clostridium) are more common in elderly patients and those with prior biliary instrumentation. Without biliary decompression, bacteremia, septic shock, multi-organ failure, and death follow.
Gallstone Pancreatitis
A stone impacting at the ampulla of Vater obstructs pancreatic duct outflow and triggers premature intrapancreatic activation of digestive enzymes — the inflammatory cascade of acute pancreatitis. Most gallstone pancreatitis episodes are mild (edematous, self-resolving in 3 to 5 days), but up to 20 percent develop severe pancreatitis with necrosis, infected necrosis, or organ failure.
Secondary Biliary Cirrhosis
Prolonged, unrelieved biliary obstruction (typically months to years, most often from benign strictures or recurrent stone disease rather than a single acute episode) causes progressive periportal fibrosis and eventually micronodular cirrhosis. Unlike alcoholic or viral cirrhosis, secondary biliary cirrhosis can reverse if the obstruction is adequately relieved early — a strong argument for prompt diagnosis and treatment.
Hepatic Abscess
Ascending cholangitis can progress to pyogenic liver abscess — pus-filled cavities within the hepatic parenchyma. Presentation includes persistent fever, RUQ pain, and tender hepatomegaly. Management requires antibiotics plus drainage (percutaneous CT-guided aspiration or surgical evacuation) in addition to biliary decompression.
Biliary Stricture
Recurrent stone passage, chronic inflammation, or complications of biliary instrumentation (post-ERCP, post-surgical) can scar and narrow the CBD, predisposing to further stone formation in a self-perpetuating cycle. Strictures may require endoscopic balloon dilation, biliary stenting, or surgical reconstruction (hepaticojejunostomy).
Recurrence
After successful CBD stone clearance:
- With gallbladder intact: recurrence rate 10 to 20 percent over 10 years (from continued stone passage)
- After cholecystectomy: much lower recurrence (residual stones from prior CBD stasis or primary stone formation; typically <5 percent at 5 years in Western populations)
- In patients with biliary strictures or primary stone disease (e.g., Oriental cholangiohepatitis): significantly higher recurrence, often requiring long-term surveillance and repeated endoscopic procedures
Research Papers
- Manes G, et al. "Systematic review and meta-analysis of endosonography versus MRCP for diagnosis of choledocholithiasis." Gastrointest Endosc. 2012;75(5):949–955. — Search PubMed
- Maple JT, et al. "The role of endoscopy in the evaluation of suspected choledocholithiasis." Gastrointest Endosc. 2010;71(1):1–9. PMID: 20105473
- Verma D, et al. "EUS vs MRCP for detection of choledocholithiasis." Gastrointest Endosc. 2006;64(2):248–254. PMID: 16860077
- Freeman ML, et al. "Complications of endoscopic biliary sphincterotomy." N Engl J Med. 1996;335(13):909–918. — Search PubMed
- Khashab MA, et al. "Pancreatic stent placement is associated with reduced risk of post-ERCP pancreatitis." Gastrointest Endosc. 2010;72(6):1202–1209. — Search PubMed
- Elmunzer BJ, et al. "A randomized trial of rectal indomethacin to prevent post-ERCP pancreatitis." N Engl J Med. 2012;366(15):1414–1422. PMID: 22494121
- Rogers SJ, et al. "Prospective randomized trial of LC+LCBDE vs ERCP/S+LC for common bile duct stone disease." Arch Surg. 2010;145(1):28–33. — Search PubMed
- Sgouros SN, et al. "Systematic review on the management of common bile duct stones." Gastrointest Endosc. 2006;63(4):620–629. — Search PubMed
- Tse F, et al. "EUS: a meta-analysis of test performance in suspected choledocholithiasis." Gastrointest Endosc. 2008;67(2):235–244. — Search PubMed
- Prat F, et al. "Prediction of common bile duct stones by noninvasive tests." Gut. 1999;44(5):702–706. — Search PubMed
- Collins C, et al. "Laparoscopic common bile duct exploration and cholecystectomy." Surg Endosc. 2004;18(12):1720–1724. — Search PubMed
- de Waele E, et al. "Choledocholithiasis: diagnosis and management 2024." Dig Endosc. 2024;36(1):18–29. — Search PubMed
Search PubMed for more: Choledocholithiasis ERCP Common bile duct stones diagnosis Post-ERCP pancreatitis prevention
Connections
- Gastroenterology
- Gallstones
- Acute Cholecystitis
- Cholangitis
- Pancreatitis
- Primary Sclerosing Cholangitis
- Gallbladder Disease