Antibiotics for E. coli Infections
Choosing the right antibiotic for an E. coli infection depends on where the infection is (bladder, kidney, or bloodstream), how sick you are, and most importantly what your local resistance rates look like. This page walks through every treatment tier in plain language — from the pills you take at home for a simple bladder infection to the IV drips used in intensive care for life-threatening sepsis. Knowing your options helps you ask better questions and avoid unnecessary side effects from drugs that are more powerful than your infection requires.
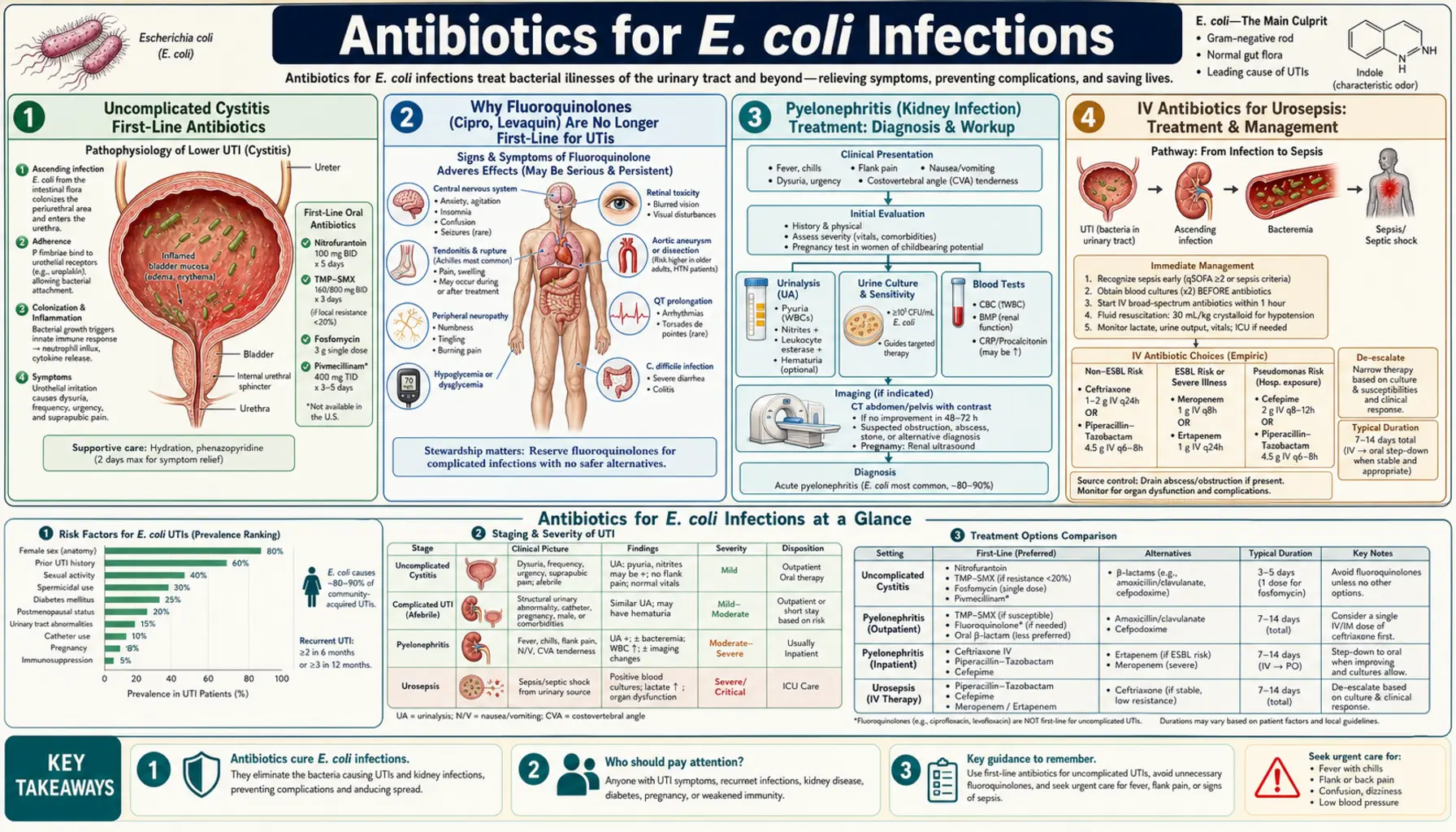
- Uncomplicated Cystitis First-Line Antibiotics
- Why Fluoroquinolones Are No Longer First-Line
- Pyelonephritis (Kidney Infection) Treatment
- IV Antibiotics for Urosepsis
- ESBL E. coli Treatment
- Never Give Antibiotics for STEC/O157:H7
- Antibiotic Resistance Rates in E. coli
- Shorter Treatment Courses: What the Evidence Shows
- Key Research Papers
- Connections
Uncomplicated Cystitis First-Line Antibiotics
An uncomplicated cystitis is a bladder infection in an otherwise healthy woman who is not pregnant, has no fever, and has no anatomical abnormalities in her urinary tract. This is the most common E. coli infection scenario, and the preferred antibiotics are specifically chosen to be effective, short-course, and less likely to disrupt the rest of your body's bacteria than broader drugs.
Nitrofurantoin (Macrobid, Macrodantin)
Dose: 100 mg of the macrocrystalline formulation (Macrobid) twice daily for 5 days. Nitrofurantoin works differently from most antibiotics — it is concentrated specifically in the urine rather than in the bloodstream, so it kills E. coli right where the infection is without affecting bacteria elsewhere in your gut or body. This is actually an advantage: it spares your good gut microbiome. Take it with food to reduce the stomach upset it can cause.
Important caution: Nitrofurantoin should be avoided if your kidneys are not working well. The threshold is an eGFR (estimated glomerular filtration rate — a measure of kidney function calculated from a blood test) below 30 mL/min/1.73m². When kidneys are impaired, not enough of the drug is concentrated into the urine to work, so you would be taking a drug that is unlikely to cure your infection. If you have chronic kidney disease, tell your doctor before they prescribe this.
TMP-SMX DS (Trimethoprim-Sulfamethoxazole, Bactrim, Septra)
Dose: One double-strength (DS) tablet twice daily for 3 days. TMP-SMX is highly effective when E. coli is susceptible to it — the short 3-day course cures uncomplicated UTI in over 90% of cases. The critical caveat is local resistance rates: if more than 20% of E. coli in your area are resistant to TMP-SMX, the drug is a poor first choice because there is too high a chance your specific infection won't respond. Resistance rates vary dramatically by geography — some US cities have rates above 20%, others are well below. Your doctor should know the local rates; if they don't, it's worth asking. Some people are allergic to sulfonamides (the "sulfa" component) — if you have had a reaction to sulfa drugs before, tell your doctor.
Fosfomycin (Monurol)
Dose: 3 grams as a single oral dose — one packet dissolved in water. The main appeal of fosfomycin is convenience: one dose, done. It works by blocking a step in bacterial cell wall construction that is different from what most other antibiotics target, so it remains active against many bacteria that resist other drugs. Resistance to fosfomycin among E. coli is still low (1–3% in the US). The main downside is cost — it is significantly more expensive than TMP-SMX or nitrofurantoin, and insurance coverage varies. It is a reasonable choice for patients who cannot tolerate the alternatives, have ESBL E. coli (see below), or who value the single-dose convenience.
Why Fluoroquinolones (Cipro, Levaquin) Are No Longer First-Line for UTIs
Fluoroquinolones — which include ciprofloxacin (Cipro), levofloxacin (Levaquin), and moxifloxacin (Avelox) — were once considered a convenient first choice for bladder infections because they work well and come as a once- or twice-daily pill. They are no longer recommended for uncomplicated UTI for two important reasons.
FDA Safety Communication (2016)
After reviewing serious adverse event reports, the US Food and Drug Administration issued a safety communication in 2016 warning that fluoroquinolones carry a risk of disabling and potentially permanent side effects that outweighs the benefit for uncomplicated infections where safer alternatives exist. These serious side effects include:
- Tendon rupture: Fluoroquinolones weaken tendons, particularly the Achilles tendon. Tendon rupture can occur during treatment or up to months after stopping the drug. The risk is highest in people over 60, those on corticosteroids, and those with kidney, heart, or lung transplants.
- Peripheral neuropathy: Damage to the nerves in the hands and feet, causing numbness, tingling, burning, or weakness. This can begin during treatment and may persist long-term or become permanent.
- Aortic dissection and aneurysm: Large population studies have found that fluoroquinolone use is associated with increased risk of tears and bulges in the aorta (the body's largest artery). This risk, while rare in absolute terms, is serious enough that these drugs should be avoided in patients with aortic disease or other risk factors.
- Central nervous system effects: Insomnia, anxiety, confusion, and in rare cases hallucinations or seizures.
Rising Resistance
E. coli resistance to ciprofloxacin has risen sharply over the past two decades, now reaching 20–30% in some US urban areas. Using fluoroquinolones for simple bladder infections also accelerates resistance development, making these drugs less effective when they are truly needed for serious infections.
When Fluoroquinolones Are Still Appropriate
Fluoroquinolones remain a legitimate choice for kidney infections (pyelonephritis) when the bacteria are confirmed susceptible and the patient cannot tolerate alternatives, and for more serious infections in hospital settings. The key principle: these are powerful drugs with real risks, reserved for situations where the benefit clearly outweighs those risks. If a doctor prescribes ciprofloxacin for a simple bladder infection, it is reasonable to ask whether nitrofurantoin, TMP-SMX, or fosfomycin would be appropriate instead.
Pyelonephritis (Kidney Infection) Treatment
Pyelonephritis means the infection has traveled up from the bladder into the kidney. The hallmark symptoms that distinguish it from a bladder infection are fever (above 38°C / 100.4°F), flank pain (pain in your side or back, under the ribs on one side), and often nausea or vomiting. Kidney infections are more serious than bladder infections and require longer treatment with drugs that achieve adequate levels not just in urine but in kidney tissue and bloodstream.
Outpatient (Mild-Moderate Illness)
Most people with pyelonephritis do not need to be admitted to the hospital if they can keep fluids and oral medication down, are not severely ill, and have no complicating factors (pregnancy, structural kidney problems, diabetes with poor control).
- Ciprofloxacin 500 mg twice daily for 7 days — the most commonly used outpatient choice when local E. coli susceptibility to fluoroquinolones is above 90%. Achieves excellent tissue levels in the kidney. Remember the side effect caveats above — this is appropriate when alternatives aren't suitable or bacteria are confirmed susceptible.
- TMP-SMX DS twice daily for 14 days — highly effective when the bacteria are susceptible. The 14-day course is longer than for bladder infections because kidney infections require more time to eradicate. Do not use TMP-SMX empirically (before culture results) if local resistance rates are above 20%.
- Oral beta-lactams (amoxicillin-clavulanate, cephalexin) are less reliably effective for pyelonephritis because they achieve lower tissue concentrations than fluoroquinolones or TMP-SMX, but they are used when other options are contraindicated.
Hospitalized Patients
If you are vomiting and cannot keep oral medication down, are severely ill with high fever and chills (rigors), or have signs of the infection spreading to the bloodstream, you will be admitted for IV antibiotics.
- IV ceftriaxone 1–2 g once daily is a common first choice — it is a broad-spectrum cephalosporin (a type of penicillin-related antibiotic) that works well against most E. coli strains and is given only once a day. The dose is 1 g for most adults, 2 g for severely ill patients.
- Step-down to oral: Once your fever has been gone for 24–48 hours and you can drink and eat without vomiting, you will switch to oral antibiotics to complete the course at home. The total course length (IV + oral combined) is typically 7–14 days guided by culture results.
IV Antibiotics for Urosepsis
Urosepsis occurs when E. coli from a urinary tract infection enters the bloodstream and triggers a dangerous systemic inflammatory response. Signs that an infection may have become sepsis include fever above 38.3°C (101°F) or low body temperature below 36°C (96.8°F), fast heart rate above 90 beats per minute, confusion, and very low blood pressure. Sepsis is a medical emergency — rapid antibiotic treatment (within one hour of recognition) significantly improves survival.
Empiric Treatment (Before Culture Results)
"Empiric" means starting a drug immediately based on what bacteria are most likely causing the infection, before the lab has had time to identify the specific organism and test which antibiotics it is susceptible to. Culture results typically take 24–48 hours.
- Ceftriaxone 1–2 g IV once daily is the most common empiric starting point for urosepsis without known risk factors for resistant bacteria. It covers most community-acquired E. coli strains.
- Piperacillin-tazobactam (Zosyn) 3.375–4.5 g IV every 6–8 hours provides broader coverage when there is concern about other gram-negative bacteria, Pseudomonas, or polymicrobial infection (multiple bacteria types). Piperacillin is a penicillin combined with tazobactam, which blocks the enzymes bacteria use to destroy it.
- Meropenem 1 g IV every 8 hours if ESBL-producing E. coli is suspected based on risk factors (recent travel to high-prevalence areas, prior ESBL infection, recent broad-spectrum antibiotic use). Meropenem is a carbapenem — the strongest class of beta-lactam antibiotics, reserved for resistant organisms.
Step-Down and De-Escalation
Once the blood culture and urine culture results return, treatment should be "de-escalated" — switched to the narrowest antibiotic that the specific bacteria is susceptible to. This is called antibiotic stewardship. Using the narrowest effective drug reduces side effects, reduces the risk of developing resistant bacteria, and preserves the effectiveness of broad-spectrum drugs for when they are truly needed. A patient started on meropenem for suspected ESBL who turns out to have a regular susceptible E. coli should be stepped down to ceftriaxone or oral TMP-SMX.
ESBL E. coli Treatment
ESBL stands for extended-spectrum beta-lactamase — an enzyme that some E. coli strains produce which destroys many common antibiotics, including most cephalosporins (ceftriaxone, ceftazidime, cefotaxime) and penicillins. To use an analogy: if a normal antibiotic is a lock that binds to the bacteria and kills it, the ESBL enzyme is a key that can break the lock before it ever reaches the bacteria. Finding ESBL on a culture report means the standard cephalosporins will not work, and the treatment plan must change.
For Severe ESBL Infections (Kidney, Bloodstream)
- Meropenem 1 g IV every 8 hours is the preferred treatment for serious ESBL E. coli infections. Carbapenems are not destroyed by the ESBL enzyme, so they work when cephalosporins fail. Meropenem is given every 8 hours in hospital.
- Ertapenem 1 g IV or IM once daily is a carbapenem that can be given just once a day and is sometimes used for outpatient IV therapy (through a home IV infusion service) once the patient is stable enough to leave the hospital. It is not active against Pseudomonas, but E. coli is not Pseudomonas, so that limitation usually does not matter.
Sparing Carbapenems: Oral Options for Uncomplicated ESBL UTI
For uncomplicated ESBL bladder infections (no fever, no kidney involvement), using a carbapenem is like using a sledgehammer for a tack. Two oral options can spare the carbapenems if the lab reports support their use:
- Fosfomycin — if the laboratory reports a minimum inhibitory concentration (MIC) of 32 mg/L or below, fosfomycin is acceptable for an uncomplicated ESBL UTI. The MIC is the lowest concentration of antibiotic that stops bacterial growth in the lab; a lower number means the drug is more potent against that particular strain.
- Nitrofurantoin — if the susceptibility report specifically shows the ESBL E. coli strain is susceptible, nitrofurantoin can be used, but only for bladder infections. It does not achieve sufficient levels in kidney tissue or blood to treat anything beyond the bladder.
Important warning about the "inoculum effect": Laboratory susceptibility tests use a standard, relatively small number of bacteria. In a real infection — especially a kidney infection or bloodstream infection — there are far more bacteria, producing far more ESBL enzyme. Cephalosporins that look "susceptible" in the lab at low bacterial numbers may fail in the body where bacterial counts are much higher. This is why doctors typically avoid cephalosporins for ESBL infections even if the lab says "susceptible."
Never Give Antibiotics for STEC / O157:H7
This is one of the most critical — and counterintuitive — rules in infectious disease management. E. coli O157:H7 and other Shiga toxin-producing E. coli (STEC) strains are the ones responsible for outbreaks linked to undercooked hamburgers, contaminated romaine lettuce, raw milk, and produce. They cause bloody diarrhea and severe abdominal cramping.
Why Antibiotics Make Things Worse
When STEC bacteria are killed by antibiotics, they release a burst of Shiga toxin — the poison that causes the most dangerous complication, hemolytic uremic syndrome (HUS). HUS is a triad of: kidney failure, destruction of red blood cells, and a dangerously low platelet count. HUS occurs in approximately 5–15% of children with STEC infections and can be fatal or cause permanent kidney damage. Studies have consistently shown that antibiotic treatment increases the risk of developing HUS — most dramatically in the landmark study by Wong et al. (2000), which showed a 17-fold higher HUS risk in antibiotic-treated children.
The Clinical Decision Point
If a patient — especially a child — presents with bloody diarrhea, severe cramping without high fever, and a history of eating undercooked ground beef, visiting a petting zoo, drinking raw milk, or eating romaine lettuce during an outbreak, STEC must be on the differential diagnosis. The correct course of action:
- Send a stool culture with specific request to test for E. coli O157:H7 and Shiga toxin (many labs do not test for this automatically).
- Hold antibiotics until STEC is excluded.
- Monitor for early signs of HUS: decreasing urine output, pallor, unusual fatigue, and bruising. These should prompt urgent blood tests including complete blood count, creatinine, and LDH (lactate dehydrogenase — a marker that rises when red blood cells are being destroyed).
- Monitoring continues for 7–10 days after illness onset — HUS typically develops 5–10 days into the illness.
Treatment of STEC infection is supportive: fluids to prevent dehydration, and careful monitoring. Antidiarrheal agents like loperamide (Imodium) should also be avoided in suspected STEC — they slow gut transit and may increase toxin absorption.
Antibiotic Resistance Rates in E. coli
Antibiotic resistance is not a future problem — it is happening now in your community. Understanding current resistance rates explains why treatment recommendations have changed and why your doctor might choose a different antibiotic than you expected.
The following figures are US community estimates; rates vary substantially by city, hospital, and patient population. Ask your healthcare provider about local rates.
- TMP-SMX: 15–25% resistance nationally in community-acquired E. coli UTI. This is why local rates must guide prescribing — TMP-SMX remains excellent if resistance is below 20%, but unreliable above that threshold.
- Ciprofloxacin: 20–30% resistance in E. coli UTI in many US urban areas, up from under 1% in 1990. This rise is largely attributable to overuse of fluoroquinolones for minor infections over the past three decades.
- Nitrofurantoin: 3–7% resistance — E. coli has been slow to develop resistance to nitrofurantoin because the drug's mechanism of action is complex and requires multiple simultaneous mutations. This low resistance rate makes it a sustainable first-line option.
- Fosfomycin: 1–3% resistance in the US — similarly low and stable, for similar reasons.
- ESBL-producing E. coli: Now causes an estimated 5–10% of community-acquired UTIs in the United States. A decade ago, ESBL E. coli was almost exclusively a hospital-acquired problem. This community spread is one of the most concerning trends in infectious disease.
- Global picture: Resistance rates are dramatically higher in South Asia, Southeast Asia, and parts of Africa. A patient who recently traveled to or lived in these regions has a much higher probability of carrying resistant E. coli. This is not a reflection on the traveler — it is a predictable consequence of higher background prevalence in those populations.
Duration of Treatment: Evidence for Shorter Courses
A common misconception is that a longer course of antibiotics is always safer or more effective. For UTIs, the evidence clearly shows that shorter courses are equally effective and produce fewer side effects. "Completing the full course" matters for some infections (like tuberculosis) where stopping early genuinely promotes resistance, but for uncomplicated UTI, shorter is better.
- TMP-SMX — 3 days vs. 7 days: Multiple randomized controlled trials have shown that 3 days of TMP-SMX is equally effective as 7 days for uncomplicated cystitis in women, with significantly fewer adverse effects (nausea, candidal vulvovaginitis, diarrhea, rash).
- Nitrofurantoin — 5 days vs. 7 days: A 5-day course of nitrofurantoin macrocrystalline achieves equivalent cure rates to 7-day courses while reducing side effects and drug exposure.
- Ciprofloxacin for pyelonephritis — 7 days vs. 14 days: For uncomplicated pyelonephritis treated with ciprofloxacin in outpatients, 7 days is equivalent to 14 days. The 14-day course has historically been used for TMP-SMX because TMP-SMX achieves lower tissue concentrations than ciprofloxacin — the choice of antibiotic determines the appropriate duration.
- The practical message: If your doctor prescribes a course that seems unusually long for a bladder infection, it is worth discussing whether a shorter evidence-based course is appropriate. Conversely, if you are treating a kidney infection or have risk factors for complicated infection, follow the recommended duration — short-course evidence applies specifically to uncomplicated bladder infections in healthy women.
Key Research Papers
- Gupta K, Hooton TM, Naber KG, et al. International clinical practice guidelines for the treatment of acute uncomplicated cystitis and pyelonephritis in women. Clin Infect Dis. 2011;52(5):e103–e120. — Search PubMed
- Sanchez GV, Babiker A, Master RN, et al. Antibiotic resistance among urinary isolates from female outpatients in the United States in 2003 and 2012. Antimicrob Agents Chemother. 2016;60(5):2680–2683. — Search PubMed
- Grigoryan L, Trautner BW, Gupta K. Diagnosis and management of urinary tract infections in the outpatient setting. JAMA. 2014;312(16):1677–1684. — Search PubMed
- Paterson DL, Bonomo RA. Extended-spectrum beta-lactamases: a clinical update. Clin Microbiol Rev. 2005;18(4):657–686. — Search PubMed
- Tamma PD, Rodriguez-Bano J. The Use of Noncarbapenem Beta-Lactams for the Treatment of Extended-Spectrum Beta-Lactamase Infections. Clin Infect Dis. 2017;64(7):972–980. — Search PubMed
- Wong CS, Jelacic S, Habeeb RL, Watkins SL, Tarr PI. The risk of the hemolytic-uremic syndrome after antibiotic treatment of Escherichia coli O157:H7 infections. N Engl J Med. 2000;342(26):1930–1936. — Search PubMed
- Gupta K, Sahm DF, Mayfield D, Stamm WE. Antimicrobial resistance among uropathogens that cause community-acquired urinary tract infections in women. Clin Infect Dis. 2001;33(1):89–94. — Search PubMed
- Cai T, Mazzoli S, Mondaini N, et al. The role of asymptomatic bacteriuria in young women with recurrent urinary tract infections: to treat or not to treat? Clin Infect Dis. 2012;55(6):771–777. — Search PubMed
- Foxman B. Urinary tract infection syndromes: occurrence, recurrence, bacteriology, risk factors, and disease burden. Infect Dis Clin North Am. 2014;28(1):1–13. — Search PubMed
- Rodriguez-Bano J, Navarro MD, Retamar P, et al. Beta-lactam/beta-lactam inhibitor combinations for the treatment of bacteremia due to extended-spectrum beta-lactamase-producing Escherichia coli. Clin Infect Dis. 2012;54(2):167–174. — Search PubMed
Search PubMed for more: E. coli UTI antibiotic treatment ESBL E. coli treatment pyelonephritis antibiotic duration
Connections
- All Bacteria
- E. coli Treatment & Prevention Hub
- E. coli UTI Symptoms
- E. coli Diagnosis and Testing
- ESBL and Carbapenem Resistance
- Food Safety and UTI Prevention
- Urinary Tract Infections